A Better Way to Breathe: Combining Allergy and Pulmonary Care Into One Clinic





Background: The use of biologic agents for severe asthma has transformed management, decreasing asthma exacerbations, improving lung function, reducing corticosteroid use, and decreasing hospitalizations. However, numerous financial and logistic barriers have complicated the implementation of biologic agents, including long wait times to see specialists and insurance coverage.
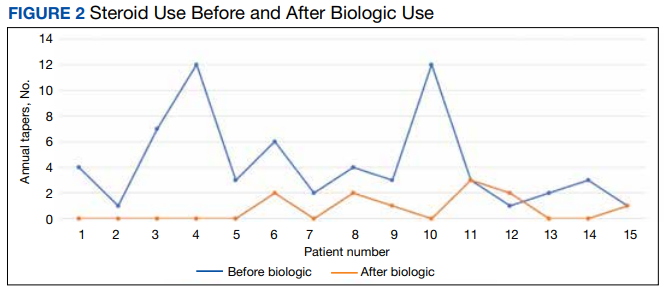
Observations: A retrospective chart review was performed for 15 patients enrolled in this severe allergy clinic at the Washington DC Veterans Affairs Medical Center over 30 months. Outcomes examined included emergency department visits, hospitalizations, intensive care unit (ICU) stays, forced expiratory volume (FEV1), and steroid use. The average use of steroids decreased from 4.2 to 0.6 tapers per year following the initiation of biologics. There was an average 10% improvement in FEV1 after starting a biologic. Thirteen percent of patients (n = 2) had an emergency department visit for an asthma exacerbation since starting a biologic agent, 0.6% of patients (n = 1) had a hospital admission for an asthma exacerbation, and no patients had an ICU stay.
Conclusions: Biologic agents have significantly improved outcomes for patients with severe asthma. The model of a combined allergy/pulmonology clinic can be particularly efficacious in the treatment of severe asthma, as it reduces the need for multiple appointments with different specialties, reduces wait time before starting a biologic agent, and offers the perspective of 2 specialists.
There was a notable clinical improvement in these patients. Before starting a biologic agent, all the patients in this study were prescribed steroids at least once a year for an asthma exacerbation, with a mean of 4.2 steroid tapers per year.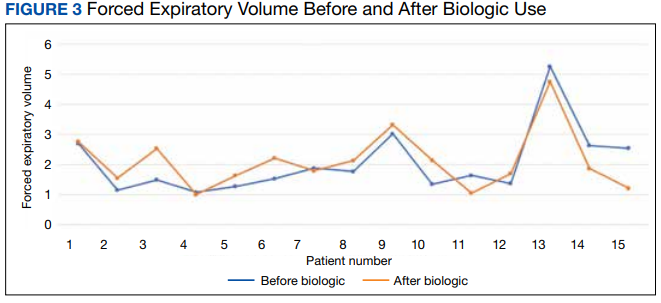
The initiation of a biologic agent also resulted in fewer ED visits and hospitalizations. Two patients had an ED visit for an asthma exacerbation since starting a biologic agent and 1 patient had a hospital admission for an asthma exacerbation. No patients were hospitalized in the ICU after starting a biologic agent.
Discussion
The 15 patients in this initial data were referred to the severe asthma clinic by pulmonology, ear, nose, and throat (ENT), primary care, and a hospitalist during an in-patient stay. As the enrollment in our clinic grows, an increasing number of patients are referred from the allergy clinic as well. Patients in the severe asthma clinic also are referred by regional centers as news of the clinic is spread by word of mouth to surrounding VA facilities. As our clinic gains the capacity to serve more patients, we hope to contact WDCVAMC primary care, pulmonology, allergy, and ENT departments to raise awareness of the clinic.
Benralizumab and dupilumab were the most used agents in this preliminary data. This finding was largely due to the ability of patients to self-administer benralizumab, which was particularly beneficial during the COVID-19 pandemic. Of note, 5 patients in this study switched from another biologic agent to benralizumab due to the ability to self-administer. Three of 5 patients that required steroids after initiating benralizumab used fewer steroids than they had previously. This finding suggests benralizumab may be the preferred agent when travel time to health care is a challenge, reducing the need for frequent clinic visits and transportation.
This preliminary data supports previous studies that have demonstrated that biologic agents improve clinical outcomes by reducing asthma exacerbations, OCS use, hospitalizations, and ICU stays for patients on all 4 biologic agents. In addition to improving patient health through avoiding complications of prolonged OCS use and hospital stays, the decrease in ED visits and hospitalizations provides a substantial cost reduction to the health care system.