Reduction of Opioid Use With Enhanced Recovery Program for Total Knee Arthroplasty





Background: Adequate pain control after total knee arthroplasty (TKA) is critically important to achieve early mobilization, shorten the length of hospital stay, and reduce postoperative complications. At Veterans Affairs North Texas Health Care System (VANTHCS) in Dallas, we implemented a multidisciplinary enhanced recovery after surgery (ERAS) protocol to deal with increasing length of stay and postoperative pain. We hypothesize that this protocol will reduce the overall opioid burden and decrease inpatient hospital length of stay in our TKA population.
Methods: A retrospective review of all TKAs performed by a single surgeon at VANTHCS from 2013 to 2018 was conducted. A postoperative ERAS protocol was implemented in 2016. We compared perioperative opioid use and LOS between cohorts before and after protocol implementation.
Results: Inpatient length of stay between cohorts was reduced from 66.8 hours for the standard of care (SOC) period to 22.3 hours in the ERAS cohort. Inpatient opioid use measured by total oral morphine equivalent doses averaged 169.5 mg and 66.7 mg for SOC and ERAS cohorts, respectively ( P = .0001). Intraoperative use of opioids decreased from 57.4 mg in the SOC cohort to 10.5 mg in the ERAS cohort ( P = .0001). Postanesthesia care unit (PACU) opioid use decreased from 13.6 mg (SOC) to 1.3 mg (ERAS) ( P = .0002). There was no significant difference in complications between cohorts ( P = .09).
Conclusions: Initiating a multidisciplinary ERAS protocol for TKA at VANTHCS significantly reduced inpatient length of stay and perioperative opioid use with no deleterious effects on complication rates. The ERAS protocol has major medical and financial implications for our unique VA population and the VA health care system.
Periarticular Injections
Intraoperatively, all patients in the SOC and ERAS groups received periarticular injections. The liposomal bupivacaine injection was added to the standard injection mixture for the ERAS group. For the SOC group, the total volume of 100 ml was divided into 10 separate 10 cc syringes, and for the ERAS group, the total volume of 140 ml was divided into 14 separate 10 cc syringes. The SOC group injections were performed with an 18-gauge needle and the periarticular soft tissues grossly infiltrated. The ERAS group injections were done with more attention to anatomical detail. Injection sites for the ERAS group included the posterior joint capsule, the medial compartment, the lateral compartment, the tibial fat pad, the quadriceps and the patellar tendon, the femoral and tibial periosteum circumferentially, and the anterior joint capsule. Each needle-stick in the ERAS group delivered 1 to 1.5 ml through a 22-gauge needle to each compartment of the knee.
Outcome Variable
The primary outcome measure was total oral MED intraoperatively, in the PACU, during the hospital inpatient stay, in the hospital discharge prescription, and during the 3-month period after hospital discharge. Incidence of nausea and vomiting during the inpatient stay and any narcotic use at 6 months postsurgery were secondary binary outcomes.
Statistical Analysis
Demographic data and the clinical characteristics for the entire group were described using the sample mean and SD for continuous variables and the frequency and percentage for categorical variables. Differences between the 2 cohorts were analyzed using a 2-independent-sample t test and Fisher exact test.
The estimation of the total oral MED throughout all phases of care was done using a separate Poisson model due to the data being not normally distributed. A log-linear regression model was used to evaluate the main effect of ERAS vs the SOC cohort on the total oral MED used. Finally, a separate multiple logistic regression model was used to estimate the odds of postoperative nausea and vomiting and narcotic use at 6 months postsurgery between the cohorts. The adjusted odds ratio (OR) was estimated from the logistic model. Age, sex, body mass index, preoperative functional independence score, narcotic use within 3 months prior to surgery, anesthesia type used (subarachnoid block with monitored anesthesia care vs general endotracheal anesthesia), and postoperative complications (yes/no) were included as covariates in each model. The length of hospital stay and the above-mentioned factors were also included as covariates in the model estimating the total oral MED during the hospital stay, on hospital discharge, during the 3-month period after hospital discharge, and at 6 months following hospital discharge.
Statistical analysis was done using SAS version 9.4. The level of significance was set at α = 0.05 (2 tailed), and we implemented the false discovery rate (FDR) procedure to control false positives over multiple tests.16
Results
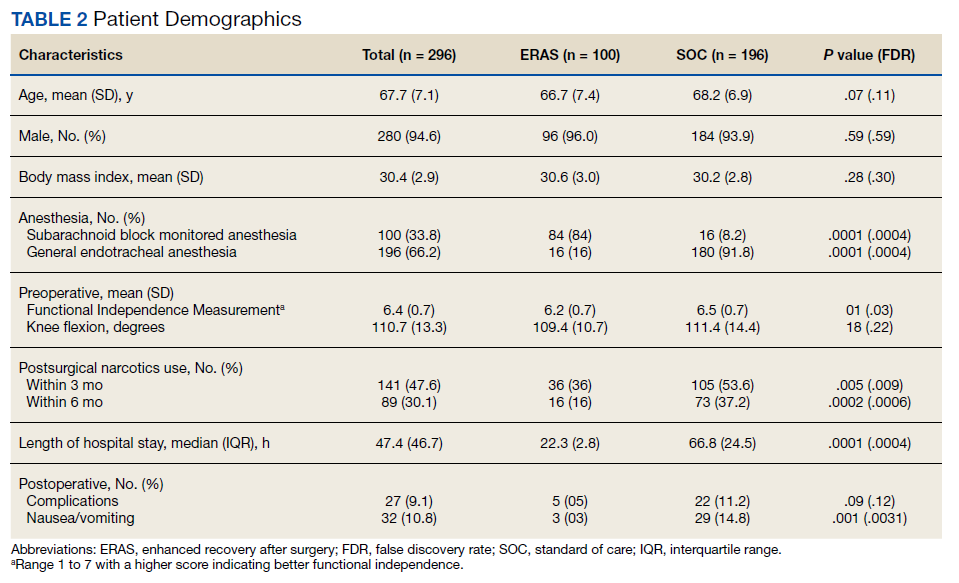
Two hundred forty-nine patients had 296 elective unilateral TKAs in this study from 2013 through 2018. Thirty-one patients had both unilateral TKAs under the SOC protocol; 5 patients had both unilateral TKAs under the ERAS protocol. Eleven of the patients who eventually had both knees replaced had 1 operation under each protocol The SOC group included 196 TKAs and the ERAS group included 100 TKAs. Of the 196 SOC patients, 94% were male. The mean age was 68.2 years (range, 48-86). The length of hospital stay ranged from 36.6 to 664.3 hours. Of the 100 ERAS patients, 96% were male (Table 2). The mean age was 66.7 years (range, 48-85). The length of hospital stay ranged from 12.5 to 45 hours.