Reduction of Opioid Use With Enhanced Recovery Program for Total Knee Arthroplasty





Background: Adequate pain control after total knee arthroplasty (TKA) is critically important to achieve early mobilization, shorten the length of hospital stay, and reduce postoperative complications. At Veterans Affairs North Texas Health Care System (VANTHCS) in Dallas, we implemented a multidisciplinary enhanced recovery after surgery (ERAS) protocol to deal with increasing length of stay and postoperative pain. We hypothesize that this protocol will reduce the overall opioid burden and decrease inpatient hospital length of stay in our TKA population.
Methods: A retrospective review of all TKAs performed by a single surgeon at VANTHCS from 2013 to 2018 was conducted. A postoperative ERAS protocol was implemented in 2016. We compared perioperative opioid use and LOS between cohorts before and after protocol implementation.
Results: Inpatient length of stay between cohorts was reduced from 66.8 hours for the standard of care (SOC) period to 22.3 hours in the ERAS cohort. Inpatient opioid use measured by total oral morphine equivalent doses averaged 169.5 mg and 66.7 mg for SOC and ERAS cohorts, respectively ( P = .0001). Intraoperative use of opioids decreased from 57.4 mg in the SOC cohort to 10.5 mg in the ERAS cohort ( P = .0001). Postanesthesia care unit (PACU) opioid use decreased from 13.6 mg (SOC) to 1.3 mg (ERAS) ( P = .0002). There was no significant difference in complications between cohorts ( P = .09).
Conclusions: Initiating a multidisciplinary ERAS protocol for TKA at VANTHCS significantly reduced inpatient length of stay and perioperative opioid use with no deleterious effects on complication rates. The ERAS protocol has major medical and financial implications for our unique VA population and the VA health care system.
Methods
A postoperative recovery protocol was implemented in 2013 at VA North Texas Health Care System (VANTHCS) in Dallas, and many of the patients continued to have issues with satisfactory pain control, prolonged length of stay, and extended opioid consumption postoperatively. A multimodal pain-management protocol and multidisciplinary perioperative case-management protocol were implemented in 2016 to further improve the clinical outcomes of patients undergoing TKA surgery. The senior surgeon (JM) organized a multidisciplinary team of health care providers to identify and implement potential solutions. This task force met weekly and consisted of surgeons, anesthesiologists, certified registered nurse anesthetists, orthopedic physician assistants, a nurse coordinator, a physical therapist, and an occupational therapist, as well as operating room, postanesthesia care unit (PACU), and surgical ward nurses. In addition, the staff from the home health agencies and social services attended the weekly meetings.
We conducted a retrospective review of all patients who had undergone unilateral TKA from 2013 to 2018 at VANTHCS. This was a consecutive, unselected cohort. All patients were under the care of a single surgeon using identical implant systems and identical surgical techniques. This study was approved by the institutional review board at VANTHCS. Patients were divided into 2 distinct and consecutive cohorts. The standard of care (SOC) group included all patients from 2013 to 2016. The ERAS group included all patients after the institution of the standardized protocol until the end of the study period.
Data on patient demographics, the American Society of Anesthesiologists risk classification, and preoperative functional status were extracted. Anesthesia techniques included either general endotracheal anesthesia or subarachnoid block with monitored anesthesia care. The quantity of the opioids given during surgery, in the PACU, during the inpatient stay, as discharge prescriptions, and as refills of the narcotic prescriptions up to 3 months postsurgery were recorded. All opioids were converted into morphine equivalent dosages (MED) in order to be properly analyzed using the statistical methodologies described in the statistical section.15 The VHA is a closed health care delivery system; therefore, all of the prescriptions ordered by surgery providers were recorded in the electronic health record.
ERAS Protocol
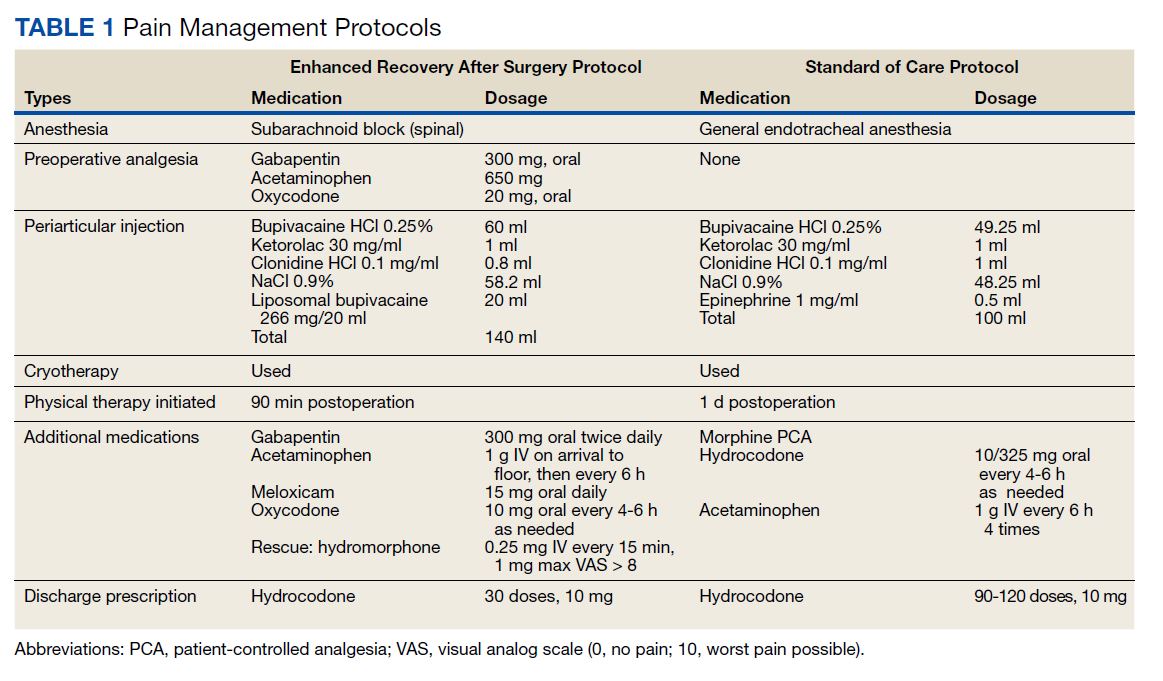
The SOC cohort was predominantly managed with general endotracheal anesthesia. The ERAS group was predominantly managed with subarachnoid blocks (Table 1). For the ERAS protocol preoperatively, the patients were administered oral gabapentin 300 mg, acetaminophen 650 mg, and oxycodone 20 mg, and IV ondansetron 4 mg. Intraoperatively, minimal opioids were used. In the PACU, the patients received dilaudid 0.25 mg IV as needed every 15 minutes for up to 1 mg/h. The nursing staff was trained to use the visual analog pain scale scores to titrate the medication. During the inpatient stay, patients received 1 g IV acetaminophen every 6 hours for 3 doses. The patients thereafter received oral acetaminophen as needed. Other medications in the multimodal pain-management protocol included gabapentin 300 mg twice daily, meloxicam 15 mg daily, and oxycodone 10 mg every 4 hours as needed. Rescue medication for insufficient pain relief was dilaudid 0.25 mg IV every 15 minutes for visual analog pain scale > 8. On discharge, the patients received a prescription of 30 tablets of hydrocodone 10 mg.