
Minimally invasive surgery in ovarian cancer






Laparoscopy has dramatically altered management of many gynecologic malignancies, but its utility in ovarian cancer has been limited—until now.
Intraoperative frozen section has high accuracy in women with metastases to the adnexae. In 36 patients with a history of breast or colorectal carcinoma who developed adnexal metastases, intraoperative frozen section correctly diagnosed carcinoma in 35 patients (97%). In more than 80% of these women, the carcinoma was accurately diagnosed as metastatic.8
Laparoscopy for Suspicious Masses?
Is laparoscopy appropriate for pelvic masses that appear suspicious for cancer at the time of preoperative evaluation? And if malignancy is confirmed, is conversion to laparotomy warranted?
Advocates of laparoscopy as the initial diagnostic tool say yes to the first question, pointing to the fact that most suspicious masses are later found to be benign.9,10
For example, Dottino et al10 managed all pelvic masses referred to their oncology unit laparoscopically unless there was evidence of gross metastatic disease (ie, omental cake) or the mass extended above the umbilicus. Immediate frozen-section analysis was performed in all cases. Although most of the masses were suspicious for malignancy preoperatively, 87% were in fact benign, and 88% were successfully managed by laparoscopy. If conversion to laparotomy was necessary for successful debulking, it was performed. However, laparoscopic surgery often was adequate.
Canis and colleagues9 support diagnostic laparoscopy regardless of the ultrasonographic appearance of the pelvic mass, although they recommend immediate conversion to laparotomy for staging if malignancy is found.
Does CO2 Sspread Cancer?
Whether CO2 contributes to cancer spread and growth is of particular concern in ovarian cancer, since it is predominantly a peritoneal disease. In a rat ovarian cancer model, tumor dissemination increased throughout the peritoneal cavity with laparoscopy, compared with laparotomy, without increased tumor growth.11
However, a separate study12 in women with persistent metastatic intraabdominal peritoneal or ovarian cancer at the time of second-look surgery found no difference in overall survival between patients who had undergone laparoscopy versus laparotomy
Fear of Port-Site Recurrence
Fear of tumor implantation at the trocar site is commonly cited as a reason to avoid laparoscopy in ovarian cancer. One metaanalysis found a port-site recurrence rate of 1.1% to 13.5%, but many of the studies included were small series or case reports.13 In ovarian cancer, most reports of port-site recurrences have been associated with advanced-stage disease with peritoneal seeding and the presence of ascites.13,14
The term “port-site recurrence” (previously it was thought to be a metastasis) describes cancer occurring in the subcutis in the absence of carcinomatosis.15 Now that the definition has been refined, the rate of port-site recurrences may be substantially lower.
A large retrospective study at our institution found 4 (0.64%) subcutaneous tumor implantations at or near a trocar site after 625 laparoscopic procedures in 584 women with ovarian/tubal cancer. Most of these implantations were discovered after positive second-look operations, and all were associated with synchronous carcinomatosis or other sites of metastatic disease.16
In a separate study14 involving 102 women with primary or recurrent advanced-stage ovarian cancer, large-volume ascites and a longer interval between chemotherapy and cytoreductive surgery were associated with more port-site recurrences. In addition, full-layer closure of the abdominal wall reduced port-site recurrences from 58% to 2%, emphasizing the importance of trocar-site closure in cases of malignancy. There was no survival disadvantage in women with portsite recurrences.
What causes port-site recurrences?
Possible factors include:
- trauma to the site,
- frequent removal of instruments through the port,
- removing the specimen through the port, and
- continued leakage of ascites.13
Avoiding cyst spillage and routinely using laparoscopic bags for cyst removal may decrease the incidence of these recurrences (FIGURE 1). Partial cyst excision and morcellation of a solid mass are always contraindicated.
Irrigation of port sites may decrease tumor cell implantation and should be considered at the end of the procedure.13 To further reduce risk, experts recommend closing all layers at the time of laparoscopy and resecting laparoscopic ports in their full thickness at the time of the staging laparotomy.14
FIGURE 1 Cyst removal using an endoscopic bag
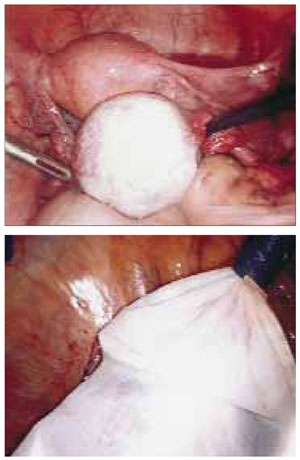
Avoid spillage and routinely use laparoscopic bags for cyst removal to decrease the incidence of port-site recurrences.
Hand-Assisted Laparoscopy
This hybrid procedure combines the advantages of minimally invasive surgery with the tactile sensation of laparotomy. It has gained favor among urologists and general surgeons. (The first nephrectomy using this method was performed in 1996.17)
Technological advances now enable the surgeon to insert and remove the nondominant hand into the peritoneal cavity without losing pneumoperitoneum and to insert instruments through the same port if needed (FIGURE 2).
Advantages over traditional laparoscopy include the ability to palpate tissue, assist with tissue retraction, perform blunt dissection, and rapidly control hemostasis. This approach has been described in management and staging of early-stage ovarian cancer and in debulking advanced disease.18
