Noninvasive vulvar lesions: An illustrated guide to diagnosis and treatment





Dystrophies, vulvodynia, and other noncancerous lesions
IN THIS ARTICLE
At least 2 vulvar pain societies—the National Vulvodynia Association and the Vulvar Pain Foundation—have newsletters, outreach programs, and Web sites.
Vulvar vestibulitis
A more readily definable condition in the same category as vulvodynia is so-called vulvar vestibulitis, also known as localized vulvodynia (as classified by the new ACOG Committee Opinion on vulvodynia).
Signs and symptoms
The defining presentation is severe pain on vestibular touch (eg, entry at intercourse), with tenderness to pressure localized within the vulvar vestibule in a horseshoe distribution pattern encompassing 3, 6, and 9 o’clock on the vestibule. Erythema is often present, especially at the 5 and 7 o’clock positions (FIGURE 3).
Patients have no symptoms during normal daily activities, but complain of dyspareunia and an inability to use tampons.
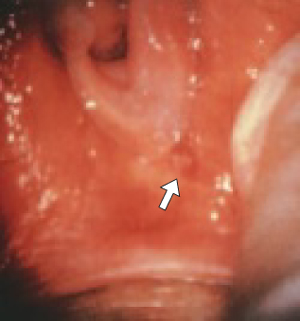
FIGURE 3
Vestibular adenitis
Intense erythema at the 5 o’clock position in the vestibule.
Diagnostic strategies
Vulvar vestibulitis can be diagnosed using a moistened cotton-tip applicator. Pressure applied in the area of the urethral meatus will result in minimal discomfort, but pressure in the horseshoe area of the vestibule will cause exquisite discomfort.
Careful inspection at 5 and 7 o’clock in the vestibule usually uncovers intense erythema over an area of 4 or 5 mm. To distinguish vestibulitis from dysesthesia, see the comparison in TABLE 1.
TABLE 1
Distinguishing vulvar vestibulitis and dysesthesia
| VULVAR VESTIBULITIS | ESSENTIAL VULVAR DYSESTHESIA |
|---|---|
| Pain is usually not constant | Pain is a constant burning sensation |
| Erythema in sensitive areas | No erythema or abnormal appearance |
| Lidocaine quells sensitivity | Lidocaine has no effect |
| Cause is dermal inflammation | Cause is allodynia (heightened nerve sensitivity) |
Recommended therapies
Treatment of vulvar vestibulitis is complex. It is important to see the patient often to ensure that this syndrome is truly present rather than vulvar dysesthesia. Xylocaine jelly should be given in an attempt to relieve symptoms; topical steroid ointments are another option.
Women with persistent symptoms are difficult to treat medically. Earlier theories pointing to infection as the cause of vestibulitis have been discounted.
Some experts believe that foods containing oxalates precipitate these symptoms. It may be advisable to have the patient reduce the content of oxalates in her diet in an effort to address all possible remedies.
For refractory cases, consider surgery
Consider surgical removal of the tender vestibule if all other therapies fail to provide adequate relief. Surgery for this indication has a high success rate (TABLE 2).7
Some surgeons have attempted treatment with laser ablation, but most have found excision more satisfactory, with faster recovery and excellent cosmesis.
Schneider and colleagues8 had 69 women complete a questionnaire 6 months after surgery, 54 (78%) of whom replied. Moderate to excellent improvement was reported by 45 women (83%); 7 had repeat surgery, after which 4 improved.
TABLE 2
Impressive track record for surgical treatment of vestibulitis
| % RESPONSE | |||
|---|---|---|---|
| STUDY | COMPLETE | PARTIAL | NONE |
| Bornstein et al7 | 76 | 24 | 0 |
| Bergeron et al12 | 63 | 37 | 0 |
| Kehoe and Luesley13 | 60 | 29 | 11 |
| Mann et al14 | 66 | 21 | 13 |
| Schover et al15 | 47 | 37 | 16 |
| Marinoff and Turner16 | 82 | 15 | 3 |
| Adapted from Bornstein et al7 | |||
Pigmented lesions
Are they cancer precursors?
Precursors of malignant melanoma of the vulva have yet to be clearly defined. The majority of these melanomas appear to arise de novo; however, some are associated with precursor nevi, especially junctional nevi. The 3 most common types of nevi that appear on the vulva are:
Assessing malignant potential
Only a small number of dysplastic nevi progress to malignant melanoma, but the frequency increases when the dysplastic nevus is familial and not acquired.
In general, the more severe the dysplasia, the greater the likelihood it will progress to malignancy. In dysplastic nevi, the pattern and appearance of the melanocytic cells are atypical. Bridging of melanocytic clusters of atypical cells may occur. Often, the atypical melanocytes are varied in size and shape, increasing in cell and nuclear size as severity increases. In the most severe cases, nucleoli are very prominent.
Many pigmented lesions of the vulva are lentigines, similar to freckles. Distinguishing one pigmented lesion from another is difficult even with magnification, and the clinician often must decide whether or not to biopsy. One set of guidelines recommends excisional biopsy of vulvar nevi when there is a change in:
Note that a reddish lesion may be basal cell hyperplasia, which has been associated with the development of basal cell carcinoma (FIGURE 4).

FIGURE 4
Basal cell carcinoma
An uncommon type of vulvar cancer, this tumor rarely metastasizes.
Premalignant lesions of squamous epithelium
The variable appearance of vulvar intraepithelial neoplasia (VIN) necessitates the liberal use of diagnostic biopsies, particularly when lesions persist or recur. VIN can present as a white lesion, or as pseudopigmented, pink, or raised and eroded.
Cigarette smoking is a risk factor.