
Electronic fetal monitoring: The difficulty of linking patterns with outcomes





Nonreassuring tracings don’t always correlate with adverse outcomes, and vice versa. A look at what we know and don’t know from evidence to date.
According to NICHD guidelines, variabilities can be defined as follows:
- amplitude undetectable = absent variability;
- amplitude of 0 to 5 beats per minute (bpm) = minimal variability;
- 5 to 25 bpm = moderate variability; and
- amplitude exceeding 25 bpm = marked variability.
Loss of variability is the most sensitive indicator of fetal acidemia, cerebral asphyxia, and myocardial depression, when it is associated with other periodic patterns.10
Baseline rate. Baseline heart rate is the approximate mean rounded to 5 bpm during a 10-minute interval, excluding periodic or episodic changes, periods of marked variability, and segments of the baseline that differ by more than 25 bpm. The baseline must continue for 2 minutes during that 10-minute period or it is considered indeterminate. A normal baseline generally ranges from 110 to 160 bpm. Below 110 bpm is bradycardia, and above 160 bpm is tachycardia.
Tachycardia and bradycardia indicate changes in the baseline rate.
Causes of tachycardia include maternal fever, sympathomimetics, and fetal arrhythmia. Tachycardia with a loss in variability and recurrent late or variable decelerations may indicate fetal acidemia.
In contrast, bradycardia ranging between 80 and 110 bpm does not indicate fetal hypoxia if the variability is retained, but a rate less than 80 bpm may indicate fetal hypoxia. The fetus may demonstrate terminal bradycardia associated with prolonged head or cord compression, but may tolerate this as long as variability is maintained. Sinusoidal patterns are excluded.
Decelerations are quantified by depth of the nadir (below the baseline) in bpm, with the duration measured in minutes or seconds from the beginning to the end of the deceleration (FIGURES 1 and 2). Those that occur more than 50% of the time are recurrent or periodic.
Acceleration is an abrupt change above baseline. Before 32 weeks, accelerations are defined as 10 or more bpm over baseline for 10 seconds or more. Peak acceleration is a minimum of 15 bpm above baseline, with a duration ranging from 15 seconds to 2 minutes before return to baseline. A prolonged acceleration continues for more than 2 minutes; if it lasts more than 10 minutes, it is considered a change in baseline.
Periodic and episodic patterns. Periodic patterns include early, late, and variable decelerations associated with uterine contractions. Episodic patterns are those not associated with uterine contractions.
A late deceleration is a visually apparent gradual decrease below the baseline for 30 seconds (at the nadir) that is delayed in timing relative to the uterine contraction. The recovery also is delayed relative to the end of the uterine contraction. Late decelerations that maintain variability are thought to indicate a well-oxygenated fetus and are neurogenic in origin,11 but late decelerations without variability are thought to represent possible asphyxia. In fetuses with prolonged placental insufficiency, these smooth late decelerations are thought to reflect decreased cerebral and myocardial function.
Early decelerations are visually apparent decreases of 30 seconds (to the nadir) that start and end with a uterine contraction. They are not associated with significant fetal acidemia.
Variable decelerations are abrupt and visually apparent decelerations of 15 bpm below the baseline; they last more than 15 seconds to the nadir and less than 2 minutes overall. Variable decelerations are generally due to head compression, vagal stimulation, or cord compression. When variable decelerations are persistent and severe, tachycardia, delayed return to baseline, or decreased variability may occur, reflecting fetal acidemia.12
Prolonged late and severe variable decelerations may lead to fetal hypoxia. A duration between 2 and 10 minutes indicates a prolonged deceleration. A change of 10 minutes or more indicates a change in baseline.
Absent or severe variability with persistent late and prolonged decelerations is generally believed to be ominous and may correlate with hypoxia of such severity that the fetal central nervous system may have already been damaged. Surrogate markers for intrapartum asphyxia include mixed acidemia at birth, low Apgar score (less than 3 at 5 minutes), seizures within 24 hours, and multiorgan dysfunction.
High-risk pattern. Fetuses at greatest risk exhibit marked bradycardia, recurrent late and variable decelerations, and absent variability.
Normal pattern. In contrast, a normal baseline with moderate variability and accelerations and absence of periodic patterns (decelerations) is predictive of fetal well-being.
Tips on interpretation. Deciphering EFM patterns entails making observations over time. Many patterns acquire increased significance when there is a trend toward persistent, significant departures from baseline with decreased variability, loss of accelerations, or persistent episodic or periodic decelerations, particularly with loss of variability.
FIGURE 2 Severe deceleration
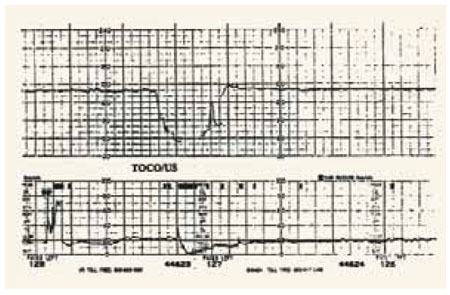
A severe deceleration with variability. When variable decelerations are persistent and severe, fetal acidemia may be present.
