Special Operations Training: An Atypical Presentation of Aspiration Pneumonia





When a 21-year-old Air Force Tactical Air Control Party trainee with no significant past medical history presented with worsening dyspnea, pleuritic chest pain, and hemoptysis, the key to a successful resolution lay in a deep and thorough patient history.
Empyema is a well-known sequela resulting from the extension of bacterial pneumonia or pulmonary abscess to the pleural space. This case highlights the organism Streptococcus intermedius (S intermedius), an uncommon cause of pulmonary empyema.1Streptococcus intermedius is endogenous among oral flora and is notorious for its abscess-forming capabilities when spread to alternative sites.
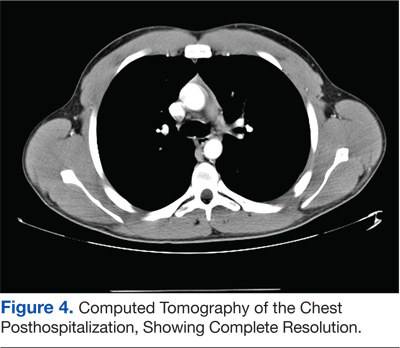
The patient was a healthy, active-duty male who presented in sepsis after months of worsening dyspnea and subacute hemoptysis following 2 near-drowning episodes during Special Operations training. Eight weeks after urgent surgical decortication and intensive antibiotic therapy, the patient experienced a complete resolution of his symptoms. A brief discussion follows concerning the pathogenesis and relevant literature regarding S intermedius infections.
Case History
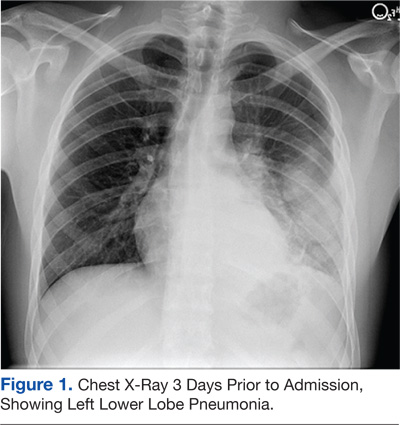
A 21-year-old Air Force Tactical Air Control Party (TACP) trainee with no significant past medical history presented with worsening dyspnea, pleuritic chest pain, and hemoptysis after failed outpatient therapy with levofloxacin for presumed community-acquired pneumonia (CAP) 3 days prior. The chest X-ray at that time demonstrated a left lower lobe consolidation with no evidence of pleural effusion or pulmonary abscess on the lateral view (Figure 1).
The patient stated that his symptoms started about 3 months prior with fever, chills, and night sweats. His symptoms occurred episodically every few weeks, but he had no knowledge of any significant events preceding the illness. The patient developed intermittent hemoptysis 2 weeks later. This included blood-streaked mucus with productive cough and bright-red blood, ranging between a teaspoon and a tablespoon, according to the patient. The patient gradually developed increased dyspnea, which began to impact his performance during Special Operations physical training. His symptoms gradually progressed to worsening dyspnea, which began to affect daily living activities, and new-onset left-sided rib pain. The patient reported no relevant travel history and tested negative for purified protein derivatives 3 months before the initial presentation.
On further questioning, the patient disclosed 2 near-drowning incidents within the preceding year. The first occurred 10 months before presentation, when the patient was performing a 1-minute underwater swim in preparation for the TACP training. The patient stated that he came to the surface to take a breath and lost consciousness. He was immediately brought to the edge of the pool and quickly recovered with no apparent residual symptoms. The second episode occurred during an underwater buddy-breathing training exercise 4 months before presentation and just 3 weeks before symptom onset. The patient reported that he knew he was not getting enough air but remained underwater, concerned that he might fail the exercise. He had a transient syncopal episode shortly after aspirating and was brought to the surface. Afterward, the patient refused to receive medical attention following this event, fearing risk of medical disqualification from training. He reportedly did not experience symptoms after this second episode.
The patient’s past medical history included seasonal allergic rhinitis, and his past surgical history was unremarkable. The patient was not taking medication other than levofloxacin, prescribed for the suspected CAP. The patient was allergic to penicillin, did not use tobacco, and reported drinking about 5 alcoholic beverages per week. His family history included a sister with asthma and a mother with factor V Leiden deficiency and pulmonary embolism related to hormone replacement therapy.
The patient’s vital signs revealed a temperature of 103.2°F, 114 beats per minute pulse, 24 breaths per minute respiratory rate, and oxygen saturation of 89% on room air. On physical examination, the patient was noted to be in moderate respiratory distress with accessory muscle use and was diaphoretic. Breath sounds were diminished in the left upper and lower lung fields with significant egophony.
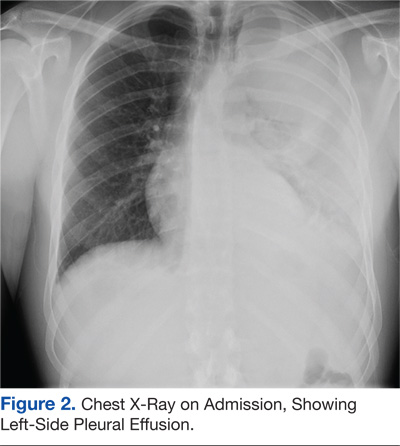
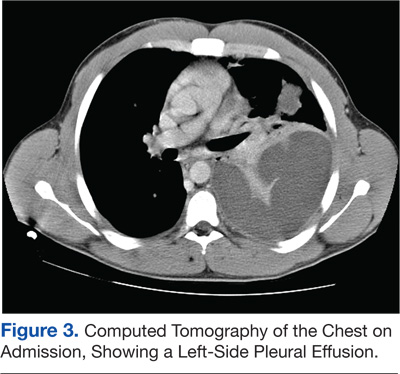
Tests revealed a white blood cell count of 23,300/mm3 with 30% bandemia. A chest radiograph showed an infiltrate/effusion of the entire left hemithorax (Figure 2). A computed tomography (CT) scan of the chest showed a large multiloculated left-side pleural effusion (Figure 3).
The patient was started on broad-spectrum antibiotics, including intravenous (IV) ceftriaxone, azithromycin, and clindamycin. He underwent thoracentesis on admission, yielding only 300 mL of purulent fluid, confirming its loculated status.
Serum total protein was 7.1 g/dL, and no serum lactic acid dehydrogenase (LDH) was obtained at the time of thoracentesis. Pleural fluid analysis revealed a protein of 5.2 g/dL, and an LDH of 5,176 units/L, meeting Light’s criteria for exudate based on a pleural fluid protein to serum protein ratio of > 0.5 (0.69) and pleural fluid LDH level > two-thirds of the upper limit of normal for serum LDH.
General surgery placed 2 thoracostomy tubes in the left hemithorax without significant drainage. On the first hospital day the patient seemed toxic and underwent a minithoracotomy with decortication. The Gram stain of the blood and blood cultures were negative over 72 hours. Another Gram stain of pleural fluid showed Gram-positive cocci in pairs. Pleural fluid cultures obtained during the procedure revealed S intermedius consistent with the patient’s history of aspiration and abscess formation. Antibiotic susceptibility tests were not performed on the sample.