Paclitaxel Drug-Drug Interactions in the Military Health System





Background: Paclitaxel is an antineoplastic agent used to treat breast, lung, endometrial, cervical, pancreatic, sarcoma, and thymoma cancer. However, drugs that induce, inhibit, or are substrates of cytochrome P450 (CYP) isoenzymes 2C8 or 3A4 may alter the metabolism of paclitaxel, potentially impacting its effectiveness. The purposes of this study are to provide an overview of paclitaxel use, identify potential drugs that interact with paclitaxel, and describe their clinical manifestations.
Methods: A retrospective analysis was performed on patients receiving paclitaxel to evaluate types and stages of cancer, treatment regimens, and adverse events of paclitaxel alone or paclitaxel in combination with other antineoplastic drugs, using data retrieved in March 2022 from the US Department of Defense Cancer Registry. Additionally, the study compared the health issues and prescriptions of patients who completed treatment with those who discontinued treatment. It evaluated interactions of paclitaxel with noncancer drugs, particularly antidepressants metabolizing and inhibiting CYP3A4, using data from the Comprehensive Ambulatory/Professional Encounter Record and the Pharmacy Data Transaction Service database. Data were retrieved in October 2022.
Results: Of 702 patients prescribed paclitaxel, 338 completed treatment. Paclitaxel discontinuation alone vs concomitantly (P < .001) and 1 drug vs combination (P < .001) both were statistically significant. Patients who took paclitaxel concomitantly with a greater number of prescription drugs had a higher rate of treatment discontinuation than those who received fewer medications. Patients in the completed group received 9 to 56 prescription drugs, and those in the discontinued group were prescribed 6 to 70. Those who discontinued treatment had more diagnosed medical issues than those who completed treatment.
Conclusions: The study provides a comprehensive overview of paclitaxel usage from 1996 through 2022 and highlights potential drug interactions that may affect treatment outcomes. While the impact of prescription drugs on paclitaxel discontinuation is uncertain, paclitaxel and antidepressants do not have significant drug-drug interactions.
RESULTS
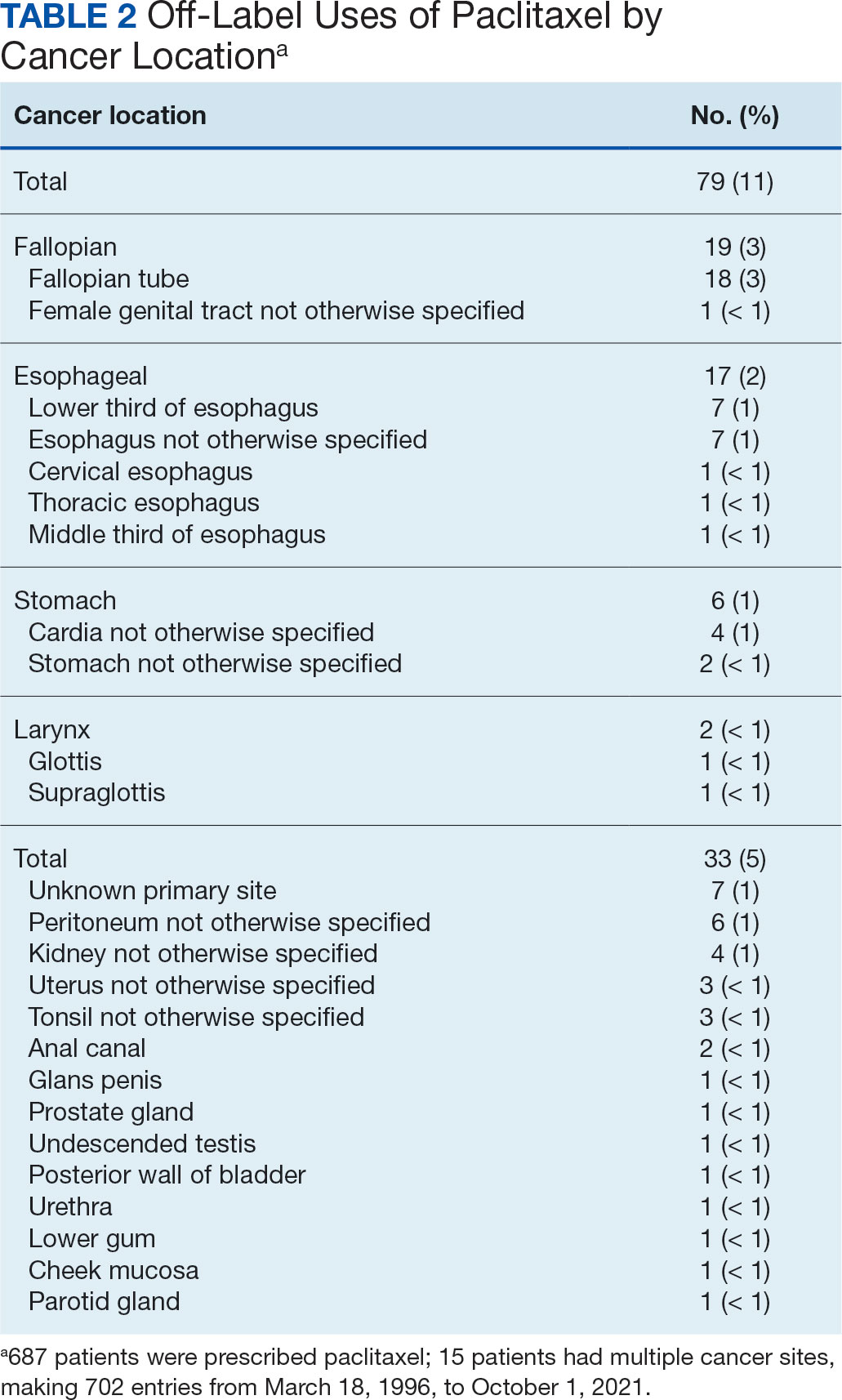
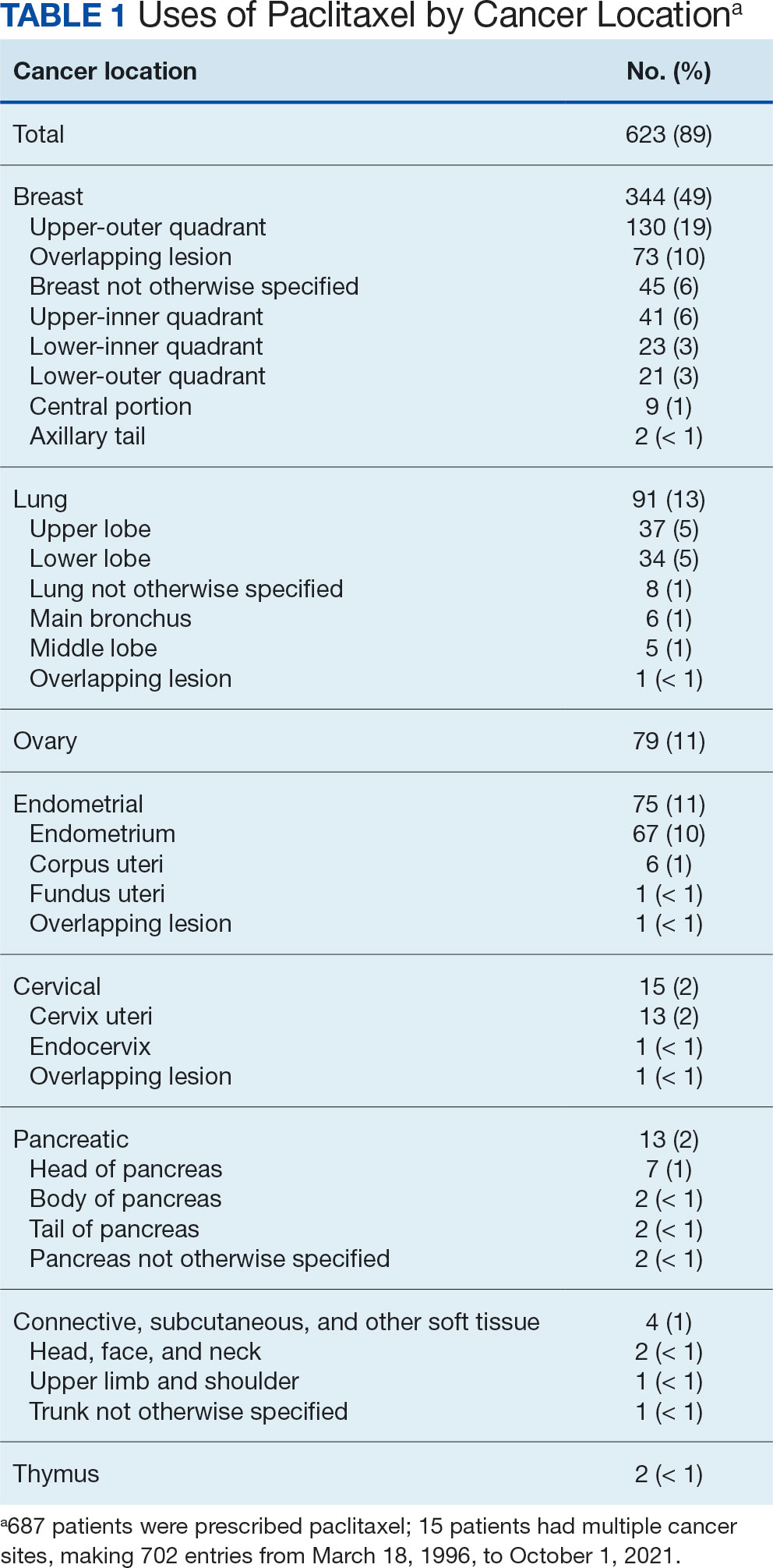
The JPC provided 702 entries for 687 patients with a mean age of 56 years (range, 2 months to 88 years) who were treated with paclitaxel from March 1996 to October 2021. Fifteen patients had duplicate entries because they had multiple cancer sites or occurrences. There were 623 patients (89%) who received paclitaxel for FDA-approved indications. The most common types of cancer identified were 344 patients with breast cancer (49%), 91 patients with lung cancer (13%), 79 patients with ovarian cancer (11%), and 75 patients with endometrial cancer (11%) (Table 1). Seventy-nine patients (11%) received paclitaxel for cancers that were not for FDA-approved indications, including 19 for cancers of the fallopian tube (3%) and 17 for esophageal cancer (2%) (Table 2).
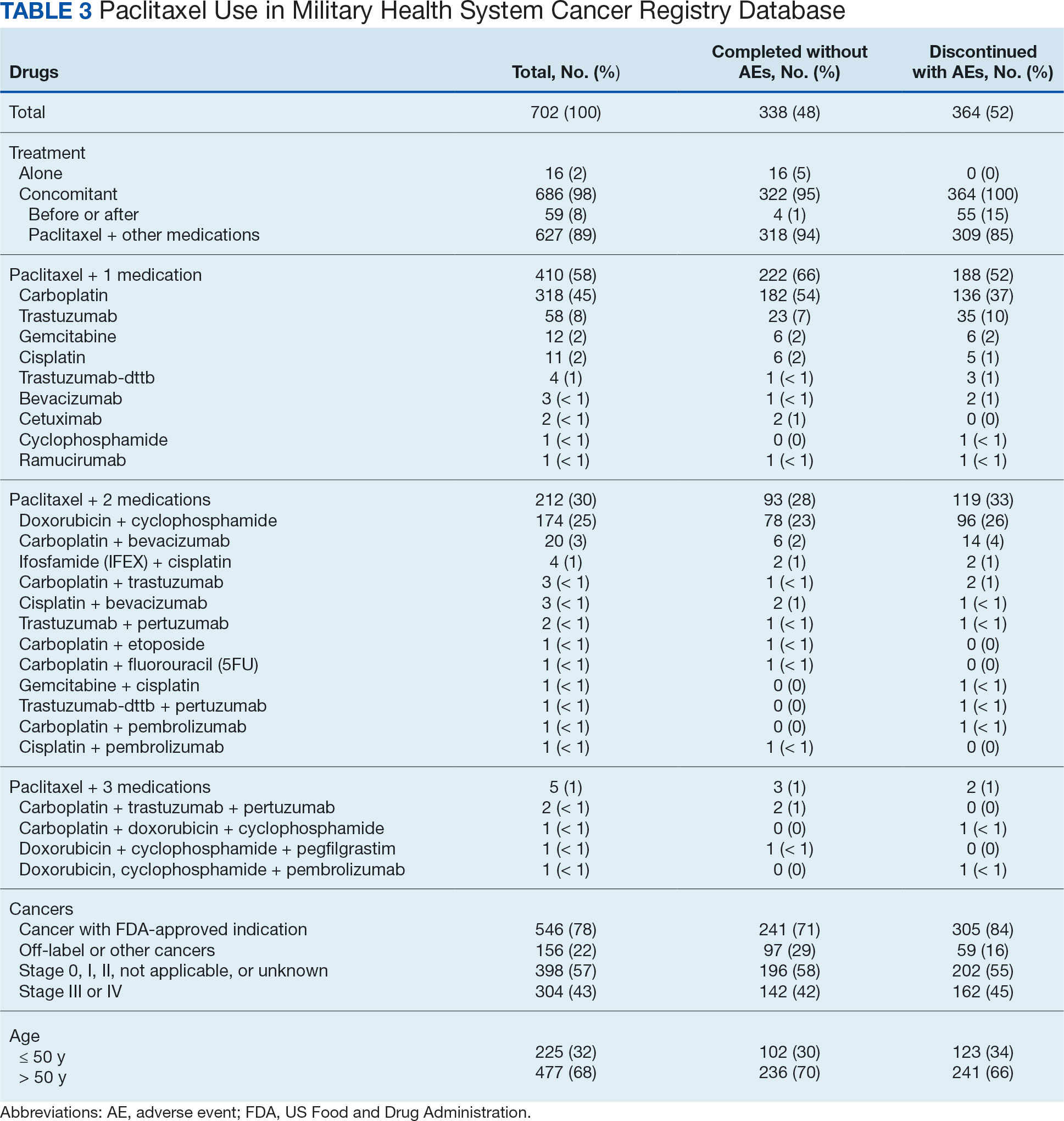
There were 477 patients (68%) aged > 50 years. A total of 304 patients (43%) had a stage III or IV cancer diagnosis and 398 (57%) had stage II or lower (combination of data for stages 0, I, and II; not applicable; and unknown) cancer diagnosis. For systemic treatment, 16 patients (2%) were treated with paclitaxel alone and 686 patients (98%) received paclitaxel concomitantly with additional chemotherapy: 59 patients (9%) in the before or after group, 410 patients (58%) had a 2-drug combination, 212 patients (30%) had a 3-drug combination, and 5 patients (1%) had a 4-drug combination. In addition, for doublet therapies, paclitaxel combined with carboplatin, trastuzumab, gemcitabine, or cisplatin had more patients (318, 58, 12, and 11, respectively) than other combinations (≤ 4 patients). For triplet therapies, paclitaxel combined withdoxorubicin plus cyclophosphamide or carboplatin plus bevacizumab had more patients (174 and 20, respectively) than other combinations, including quadruplet therapies (≤ 4 patients) (Table 3).
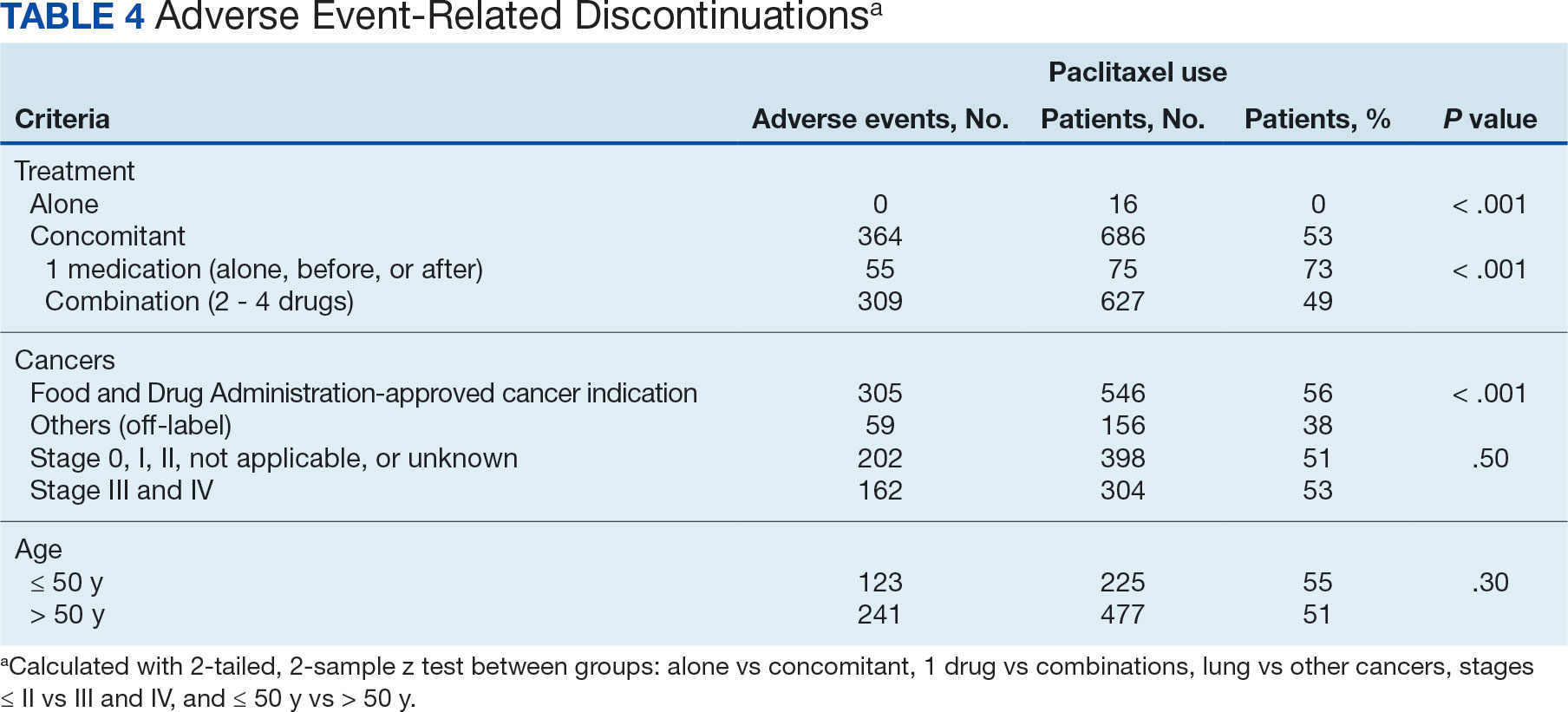
Patients were more likely to discontinue paclitaxel if they received concomitant treatment. None of the 16 patients receiving paclitaxel monotherapy experienced AEs, whereas 364 of 686 patients (53%) treated concomitantly discontinued (P < .001). Comparisons of 1 drug vs combination (2 to 4 drugs) and use for treating cancers that were FDA-approved indications vs off-label use were significant (P < .001), whereas comparisons of stage II or lower vs stage III and IV cancer and of those aged ≤ 50 years vs aged > 50 years were not significant (P = .50 andP = .30, respectively) (Table 4).
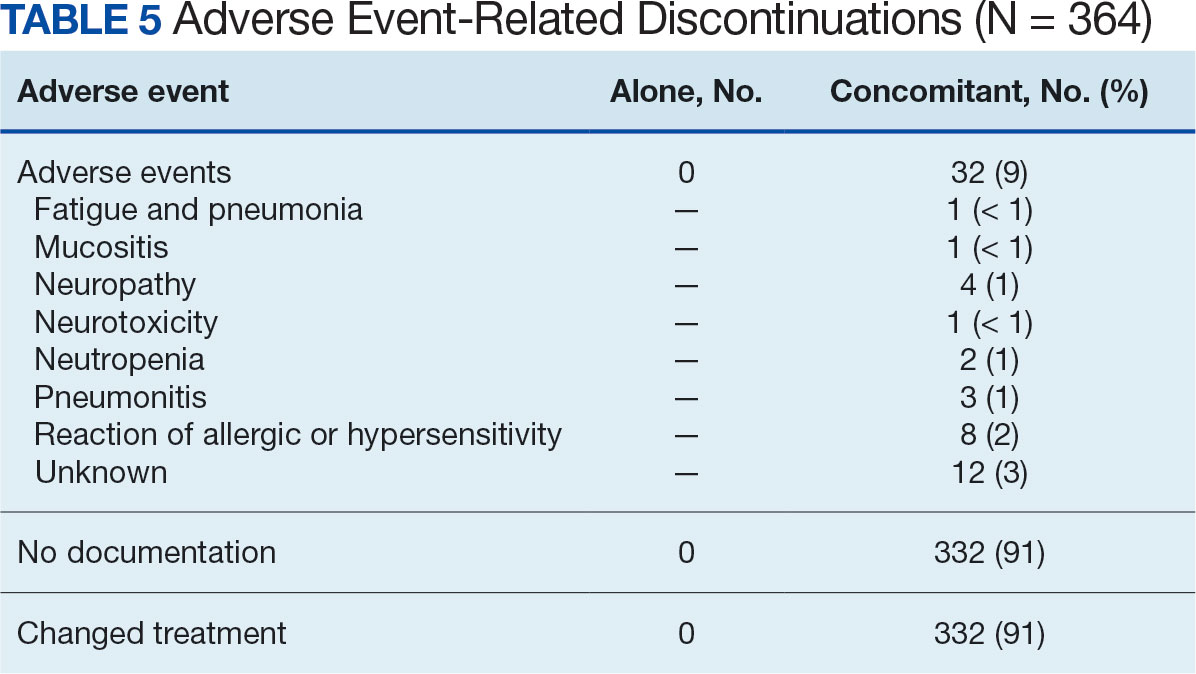
Among the 364 patients who had concomitant treatment and had discontinued their treatment, 332 (91%) switched treatments with no AEs documented and 32 (9%) experienced fatigue with pneumonia, mucositis, neuropathy, neurotoxicity, neutropenia, pneumonitis, allergic or hypersensitivity reaction, or an unknown AE. Patients who discontinued treatment because of unknown AEs had a physician’s note that detailed progressive disease, a significant decline in performance status, and another unknown adverse effect due to a previous sinus tract infection and infectious colitis (Table 5).
Management Analysis and Reporting Tool Database
MHS data analysts provided data on diagnoses for 639 patients among 687 submitteddiagnoses, with 294 patients completing and 345 discontinuing paclitaxel treatment. Patients in the completed treatment group had 3 to 258 unique health conditions documented, while patients in the discontinued treatment group had 4 to 181 unique health conditions documented. The MHS reported 3808 unique diagnosis conditions for the completed group and 3714 for the discontinued group (P = .02).