Kikuchi-Fujimoto Disease: A Case Report of Fever and Lymphadenopathy in a Young White Man





Background: Kikuchi-Fujimoto disease (KFD) is a rare cause of rapidly evolving tender cervical lymphadenopathy. It is often initially misdiagnosed and managed as infectious lymphadenitis. Although most cases of KFD are self-limited and improve with antipyretics and analgesics, some are more refractory and may require corticosteroids or hydroxychloroquine therapy.
Case Presentation: A 27-year-old White man presented for evaluation of fevers and painful cervical lymphadenopathy. He was found to have KFD on excisional lymph node biopsy. His symptoms proved challenging to manage with corticosteroids but eventually improved with hydroxychloroquine monotherapy.
Conclusions: KFD diagnosis should be considered irrespective of geographic location, ethnicity, or patient sex. Hepatosplenomegaly is a relatively rare manifestation of KFD that can make it especially difficult to distinguish from lymphoproliferative disorder, such as lymphoma. Lymph node biopsy is the preferred diagnostic approach to achieve a timely and definitive diagnosis. Although usually self-limited, KFD has been associated with autoimmune conditions, including systemic lupus erythematosus. Securing the diagnosis of KFD is therefore crucial to ensuring patients are monitored appropriately for the development of associated autoimmune conditions.
Computed tomography (CT) of the neck revealed multiple heterogeneously enlarged lymph nodes along the right anterior cervical chain with necrotic changes (Figure 1).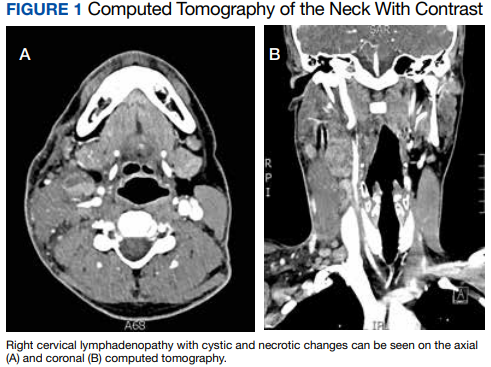
A core needle biopsy of a right-sided cervical lymph node was initially pursued, demonstrating necrotic tissue with minimal residual lymphoid tissue and no definitive evidence of lymphoma. Because these results were nondiagnostic, an excisional biopsy of the right-sided cervical lymph node was pursued 10 days later. Due to the stress of his 2-week hospitalization without a unifying diagnosis, the patient then elected to discharge home with close outpatient follow-up while awaiting his biopsy results. Antibiotics were not continued at the time of discharge as our broad infectious workup failed to yield a causative organism.
Two weeks postdischarge, the patient’s excisional lymph node biopsy returned demonstrating lymphohistiocytic inflammation with plasmacytoid dendritic cells, areas of necrosis, and scattered karyorrhectic nuclear debris, consistent with a diagnosis of KFD (Figure 2).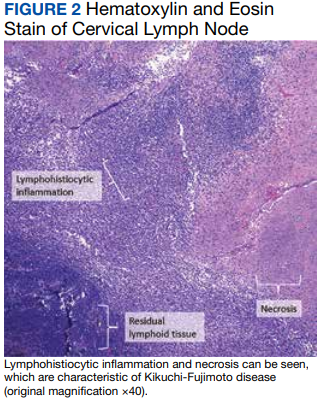
After 4 months of hydroxychloroquine therapy, the patient’s KFD symptoms resolved, prompting his dose to be reduced and eventually tapered. Repeat testing of his ANA and anti-dsDNA were performed at 1 and 6 months posthospitalization and returned within normal limits. A repeat PET-CT was performed 6 months posthospitalization showing resolution of his hypermetabolic right neck and right supraclavicular lymphadenopathy as well as his splenomegaly. It has now been more than a year since the patient’s initial presentation to the hospital, and he remains symptom-free and off prednisone and hydroxychloroquine.