Contralateral Constrictor Dose Predicts Swallowing Function After Radiation for Head and Neck Cancer





Background: Radiation therapy can cause long-term dysphagia that seriously affects quality of life for survivors of head and neck cancer. This study evaluates a novel organ at risk, the contralateral pharyngeal constrictor muscles, to find out whether radiation dose to this structure predicts late swallowing function in patients with head and neck cancer.
Methods: The study included patients with head and neck cancer treated with radiation and concurrent systemic therapy at a single institution over 3 years. One-year dysphagia was defined as either the presence of a gastrostomy tube or an abnormal modified barium swallow ≥ 1 year after completion of radiation.
Results: Fifty-five patients met inclusion criteria, of which 46 were alive at 1 year. One-year dysphagia was present in 37% (n = 17) of this population. Contralateral constrictor V60 < 40% was associated with a 1-year dysphagia rate of 6%, compared with 57% in patients with V60 ≥ 40% (P < .001). An uninvolved pharynx mean dose < 45 Gy was associated with a 1-year dysphagia rate of 22%, compared with 52% in patients with an uninvolved pharynx mean dose ≥ 45 Gy (P = .03). Editing the clinical target volume off air cavities was associated with a decrease in 1-year dysphagia from 67% to 12% (P < .001), and with a reduction of contralateral constrictor V60 from 62% to 33% (P < .001). Air cavity editing was not associated with a change in locoregional recurrence or 1-year survival.
Conclusions: This is the first study to report a connection between contralateral constrictor dose and late swallowing function. The correlation between air cavity editing and contralateral constrictor V60 suggests that contralateral constrictor dose may depend partly on technique. Further studies are needed to explore whether these findings can be replicated prospectively and in other practice settings.
Discussion
This is the first study to link contralateral constrictor dose to long-term dysphagia in patients treated with radiation for H&N cancer. Editing the boost volume off air cavities was associated with lower contralateral constrictor V60 and with less long-term dysphagia. This may indicate that optimizing plans to meet a contralateral constrictor constraint can reduce rates of long-term dysphagia.
The most useful clinical predictors are those that identify a patient at low risk for toxicity. These constraints are useful because they reassure physicians that treatments will have a favorable risk/benefit ratio while identifying plans that may need modification before starting treatment.
The contralateral constrictor outperformed the uninvolved pharynx in identifying patients at low risk for long-term dysphagia. This difference could not be overcome by decreasing the threshold of the pharynx constraint, as 17% of patients with dysphagia had a mean dose of < 40 Gy to the uninvolved pharynx, which was not statistically significant.
An advantage of contralateral constrictor is that it is independent of planning target volume (PTV) size. The uninvolved pharynx structure depends on the PTV contour, so it may obscure a connection between PTV size and dysphagia.
In the context of a clinical trial, only measuring dose to the uninvolved pharynx may allow more plans to meet constraints, but even in NRG trials, physicians have some control over target volumes. For example, NRG HN009, a national trial for patients with H&N cancer, recommends editing the CTV_7000 (clinical target volume treated to 70 Gy) off air cavities but does not define how much the volume should be cropped or specify protocol violations if the volume is not cropped.15 Furthermore, constraints used in clinical trials are often adopted for use outside the trial, where physicians have extensive control over target volumes.
The broad range of uninvolved pharynx volume relative to total constrictor volume confounds predictions using this variable. For example, according to the NRG constraint, a patient with an uninvolved pharynx mean dose of 44 Gy will have a low risk of dysphagia even if this structure is only 1% of the total constrictor. The contralateral constrictor is always about 50% of the total constrictor volume, which means that predictions using this structure will not be confounded by the same variation in volume size.
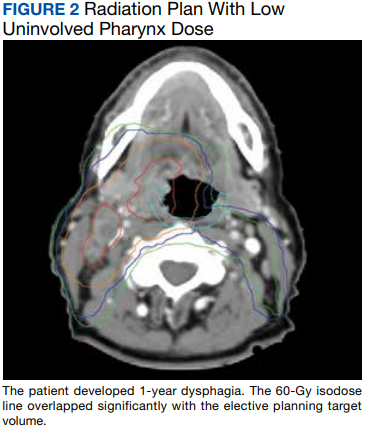
Figure 2 shows a representative patient who met the NRG uninvolved pharynx constraint but developed long-term dysphagia.