Daniel Liaou, MDa,b; Patrick N. O’Mahen, PhDa,c; Laura A. Petersen, MD, MPHa,c Correspondence: Laura Petersen (laurap@bcm.edu)
aCenter for Innovations in Quality, Effectiveness, and Safety, Michael E. DeBakey Veterans Affairs Medical Center, Houston, Texas bDepartment of Psychiatry and Behavioral Sciences, McGovern Medical School, UTHealth Houston, Texas cSection for Health Services Research, Department of Medicine, Baylor College of Medicine, Houston, Texas
Author disclosures
The authors report no financial conflicts of interest. This work was supported by the US Department of Veterans Affairs (VA), Veterans Health Administration, Office of Research and Development, and the Center for Innovations in Quality, Effectiveness and Safety (CIN-13-413). Support for VA/CMS data provided by the Department of Veterans Affairs, VA Health Services Research and Development Service, VA Information Resource Center (Project Numbers SDR 02-237 and 98-004). These institutions played no role in the design of the study or the analysis of the data.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner , Frontline Medical Communications Inc., the US Government, or any of its agencies.
Ethics and consent
Our protocol (#H-40441) was reviewed and approved by the Baylor College of Medicine Institutional Review Board, which waived the informed consent requirement. This study was approved by the Michael E. DeBakey Veterans Affairs Medical Center Research and Development Committee.
Background: In 2001, before the Affordable Care Act (ACA), some states expanded Medicaid coverage to include an array of mental health services, changing veterans’ reliance on US Department of Veterans Affairs (VA) services.
Methods: Using Medicaid and VA administrative data from 1999 to 2006, we used a difference-in-difference design to calculate shifts in veterans’ reliance on the VA for depression care in New York and Arizona after the 2 states expanded Medicaid coverage to adults in 2001. Demographically matched, neighbor states Pennsylvania and New Mexico/Nevada were used as paired comparisons, respectively. Fractional logit was used to capture the distribution of inpatient and outpatient depression care utilization between the VA and Medicaid, while ordered logit and negative binomial regressions were applied to model Medicaid-VA dual users and per capita utilization of total depression care services, respectively.
Results: Medicaid expansion was associated with a 9.50 percentage point (pp) decrease (95% CI, -14.61 to -4.38) in reliance on the VA for inpatient depression care among service-connected veterans and a 13.37 pp decrease (95% CI, -21.12 to -5.61) among income-eligible veterans. For outpatient depression care, VA reliance decreased by 2.19 pp (95% CI, -3.46 to -0.93) among income-eligible veterans. Changes among service-connected veterans were nonsignificant (-0.60 pp; 95% CI, -1.40 to 0.21).
Conclusions: After Medicaid expansion, veterans shifted depression care away from the VA, with effects varying by health care setting, income- vs service-related eligibility, and state of residence. Issues of overall cost, care coordination, and clinical outcomes deserve further study in the ACA era of Medicaid expansions.
This project was approved by the Baylor College of Medicine Institutional Review Board (IRB # H-40441) and the Michael E. Debakey Veterans Affairs Medical Center Research and Development Committee.
Results
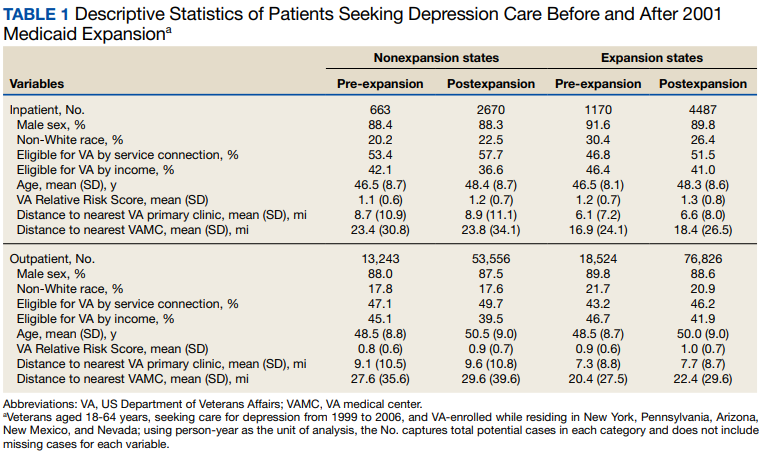
Baseline and postexpansion characteristics
for expansion and nonexpansion states are reported in Table 1. Except for non-White race, where the table shows an increase in nonexpansion to expansion states, these data indicate similar shifts in covariates from pre- to postexpansion periods, which supports the parallel trends assumption. Missing cases were less than 5% for all variables.
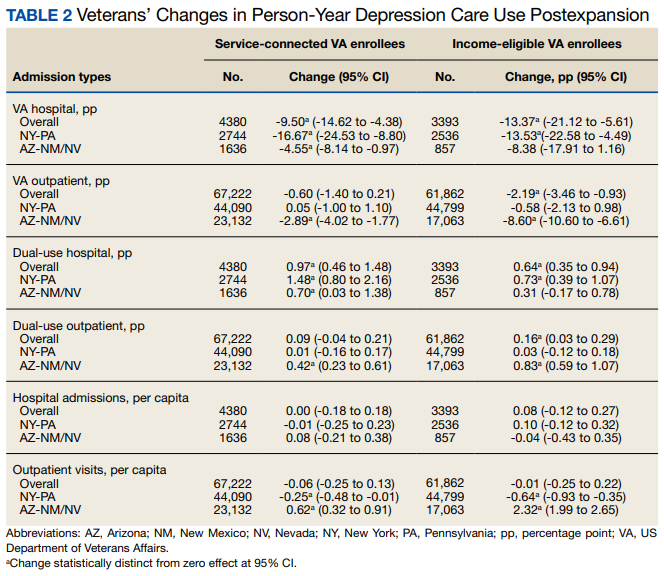
VA Reliance
Overall, we observed postexpansion decreases in VA reliance for depression care
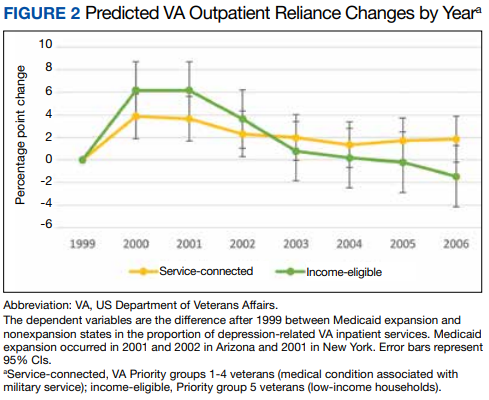
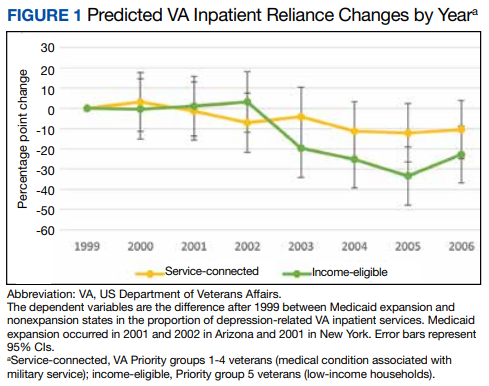
among expansion states compared with nonexpansion states (Table 2). For the inpatient analysis, Medicaid expansion was associated with a 9.50 percentage point (pp) relative decrease (95% CI, -14.62 to -4.38) in VA reliance for depression care among service-connected veterans and a 13.37 pp (95% CI, -21.12 to -5.61) decrease among income-eligible veterans. For the outpatient analysis, we found a small but statistically significant decrease in VA reliance for income-eligible veterans (-2.19 pp; 95% CI, -3.46 to -0.93) that was not observed for service-connected veterans (-0.60 pp; 95% CI, -1.40 to 0.21). Figure 1 shows
adjusted annual changes in VA reliance among inpatient groups, while Figure 2 highlights outpatient groups. Note also that both the income-eligible and service-connected groups have similar trend lines from 1999 through 2001 when the initial ound of Medicaid expansion happened, additional evidence supporting the parallel trends assumption.