Improving Unadjusted and Adjusted Mortality With an Early Warning Sepsis System in the Emergency Department and Inpatient Wards





Background: Mortality reduction has been a major focus of improvement for health care systems. Although several studies have noted improved sepsis-related mortality with the use of electronic health record (EHR) systems, there are no known published early warning sepsis systems using the Veterans Health Administration (VHA) EHR system.
Methods: The Malcom Randall Veterans Affairs Medical Center (MRVAMC), a large academic 1a VHA facility within the North Florida/South Georgia Veterans Health System (NF/SGVHS), was identified as having opportunities for improvement related to inpatient mortality outcomes. Sepsis was discovered as the primary contributor to inpatient mortality for MRVAMC’s acute level of care (LOC). Education along with implementation of an early warning sepsis system (EWSS) was subsequently integrated in the VHA EHR known as the Veterans Information Systems and Technology Architecture/Computerized Patient Record System (VistA/CPRS) at NF/SGVHS, which applied a combination of informatics solutions within a Lean Six Sigma quality improvement framework.
Results: At MRVAMC, there was an observed decrease in the number of inpatient deaths for the acute LOC from a high of 48 in fiscal year (FY) 2017, quarter 3 to a low of 27 in FY 2019, quarter 4. This resulted in as large of an improvement as a 44% reduction in unadjusted mortality with education and implementation of an EWSS from FYs 2017 to 2019. Additionally, the MRVAMC acute LOC risk-adjusted mortality (standardized mortality ratio) improved from > 1.0 to < 1.0, demonstrating fewer inpatient mortalities than predicted from FYs 2017 to 2019.
Conclusions: Education along with the possible implementation of an EWSS within the VHA EHR was associated with improvement in unadjusted and adjusted inpatient mortality at MRVAMC. This may be an effective approach for patients with sepsis.
The number of MRVAMC inpatient deaths increased from 28 in FY 2018, quarter 1 to 45 in FY 2018, quarter 3. While acute LOC showed improvement in unadjusted mortality after sepsis education/awareness, it was felt continuous improvement could not be sustained with education alone. An EWSS was designed and implemented within the EHR system in FY 2018. Following implementation of EWSS and reeducating staff on early recognition and treatment of sepsis, acute LOC inpatient deaths decreased from 45 in FY 2018, quarter 3 through FY 2019 where unadjusted mortality was as low as 27 during FY 2019, quarter 4. The MRVAMC acute LOC SMR was consistently < 1.0 from FY 2018, quarter 4 through FY 2019, quarter 4.
In addition to the observed decrease in acute LOC inpatient deaths and improved SMR, the number of ERT alerts and sepsis alerts on the inpatient wards were monitored from FY 2017 through FY 2019. ERT alerts listed in Table 3 were nonspecific and initiated by nursing staff on the wards where a patient’s clinical status was identified as worsening while sepsis alerts were specific ERT alerts called by the ward nursing staff due to concerns for sepsis. The inpatient wards included inpatient medicine, surgery, and psychiatry acute care and the intermediate level of care unit while outpatient clinical areas of treatment, intensive care units, stroke alerts, and STEMI alerts were excluded.
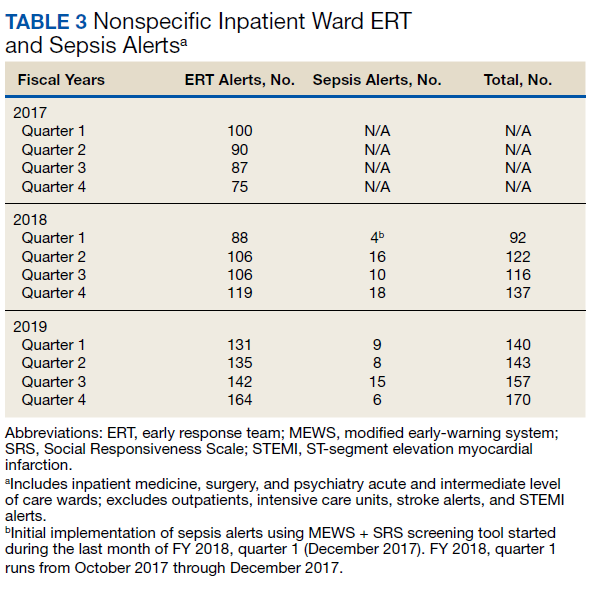
From FY 2017 to FY 2018, quarter 1, the number of nonspecific ERT alerts varied between 75 to 100. Sepsis alerts were not available until December 2017 while the EWSS was in development. Afterward, nonspecific ERT alerts and sepsis alerts were monitored each quarter. Sepsis alerts ranged from 4 to 18. Nonspecific ERT alerts + sepsis alerts continued to increase from FY 2018, quarter 3 through FY 2019, quarter 4.
Discussion
Implementation of the EWSS was associated with improved unadjusted mortality and adjusted mortality for acute LOC at MRVAMC. Although variation exists with application of EWSS at other medical centers, there was similarity with improved sepsis outcomes reported at other health care systems after EWSS implementation.7-16
Improved unadjusted mortality and adjusted mortality for acute LOC at MRVAMC was likely due to multiple contributing factors. First, during design and implementation of the EWSS, project work was interdisciplinary with input from physicians, nurses, and pharmacists from multiple specialties (ie, ED, ICU, and the medicine service); quality management and data analysis specialists; and clinical informatics. Second, facility commitment to improving early recognition and treatment of sepsis from leadership level down to front-line staff was evident. Weekly sepsis meetings with the NF/SGVHS chief of staff helped to sustain EWSS efforts and to identify additional improvement opportunities. Third, integrated informatics solutions within the EHR helped identify early sepsis and minimized human error as well as assisted with coordination of sepsis care across services. Fourth, the focus was on both early identification and treatment of sepsis in the ED and hospital wards. Although it cannot be deduced whether there was causation between reduced inpatient mortality and an increased number of nonspecific ERT alerts+ sepsis alerts on the inpatient wards after EWSS implementation, inpatient deaths decreased and SMR improved. Finally, the EWSS emphasized both the importance of evidence-based clinical care of sepsis and standardized documentation to appropriately capture clinical severity of illness.
