Operational Curriculum and Research Initiatives: Shaping the Future of Military Medicine





Background: The current operational tempo and transitions in the structure of the military health system demands a renewed commitment to operational medicine readiness. There is an official mandate as well as the practical necessity to increase operational readiness within the medical corps. There is also a need to continue the scholarly evaluation of military medicine through research to ensure the progression of evidence-based medical care for the war fighter. Military graduate medical education (GME) has been threatened by budget cuts and lack of understanding of its value. This article reviews the literature on operational medicine curriculums and makes recommendations to restructure current military medicine training to produce operationally prepared clinicians who are informed in operationally focused research principles.
Observations: During early medical training operational curriculum cements military identity, fosters military leadership skills, provides practice of scenarios unique to military medicine, and connects learners to experienced mentors. There have been several versions of curriculum development in various GME programs observed from a literature search; however, the curriculum overall is fragmented and there is no universal implementation. Studies have shown that deliberately mapped longitudinal curriculums can be well integrated into a existing medical curriculum. Multiple studies also suggest that military GME is a large component of the production of operational-themed medical research and is vital for continued advancements. Value-based analysis performed by multiple sources have found that the initial increased cost of a military medical school education and GME becomes cost-effective based on increased retention, deployments, and filling of leadership billets.
Conclusions: Access to existing operational training structures that have well-established programs should be increased, and individual GME program curriculums should be modeled on those that have shown proven success with a focus on operational training, leadership, and research.
Didactics can provide a foundation. However, just as the practice of medicine is learned in the clinic, the art of military medicine is learned in the field. Hands-on training in one study was accomplished through the Combat Casualty Care Course (C4), the USU Bushmaster exercise, and a field training exercise. The field exercise included components of mission planning, medical threat assessments, triage of a mass casualty situation, management of disease and nonbattle injuries, combat stress casualties, resource management, and patient evacuation.8
Another publication described a similar longitudinal curriculum with C4 after the first year of training and the Medical Management of Chemical and Biological Casualty Course during the second year. The operational curriculum 3-day capstone occurred at the end of medical training utilizing mannequins to realistically simulate combat casualty care, including emergency airways, chest tube, and tourniquets.9 Due to the current deployment tempo, just in time refresher courses like this could be valuable preparation.
While most of the operational curriculums evaluated assessed efficiency over a short time interval, one study looked at 1189 graduates from the military medical school from the past 20 years. Preparedness was perceived to be high for military-unique practice and leadership.10 The operational curriculum at USU had been purposefully structured to provide continuity. Didactics and casework were reinforced with hands-on training whether through realistic simulator training or field exercises. The authors note a weakness of many operational curriculums is inconsistency and fragmented training without deliberate longitudinal planning.
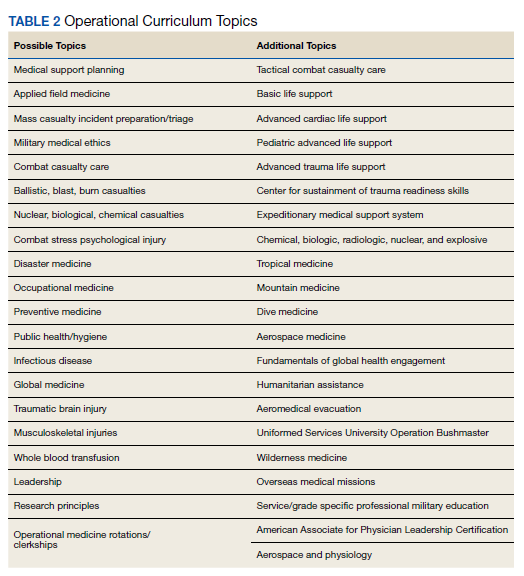
One of the more recent military GME curriculums include the creation of the operational medicine residency in 2013, which created a standardized longitudinal operational curriculum integrated along with the existing family medicine, emergency medicine, or internal medicine curriculum to create mission-ready military physicians upon graduation. Scheduled rotations include global medicine, aeromedical evacuation, occupational medicine, and tropical medicine. Completing military officer professional development and an operationally relevant research project is an expectation (Table 2).11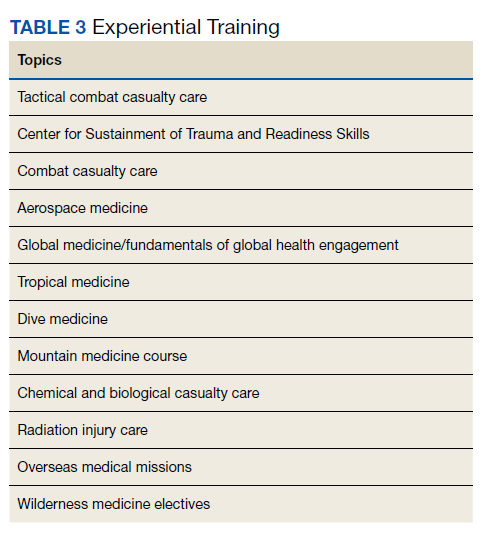
In addition to in-program training, other options include operational rotations offsite and military courses conducted outside the GME program.12 Some of these courses may include just-in-time training such as expeditionary medical support system training prior to scheduled deployments. Examples of experiential training are listed in Table 3.
Critical Analysis
Current gaps were identified in the military medicine training pipeline’s operational medicine curriculum and research programs. The analysis looked at specific components that make the operational medicine curriculum and research unique as well as current readiness goals, to determine how to best align both to meet the mission requirements. Some factors considered included efficiency, cost, program portability, duplication minimization, retention, and sustainability.