Opioid Management in Older Adults: Lessons Learned From a Geriatric Patient-Centered Medical Home





Background: The United States continues to confront an opioid crisis that also affects older adults. Best practices for prescription opioid management in older adults are challenging to implement in this population. We present our experience with a 1-year management of 48 high-risk older patients who received guideline-based best practices for chronic prescription opioid therapy at a US Department of Veterans Affairs (VA) patient aligned care team (PACT) patient-centered medical home.
Methods: The GeriPACT population at the Nashville Campus of the VA Tennessee Valley Healthcare System has an enrollment of 745 patients of whom 48 (6.5%) receive chronic prescription opioid therapy. The practice is supported by the VA Computerized Patients Record System, including the electronic patient portal, My health e Vet, and telemedicine capabilities. Data were collected by chart review and operations data.
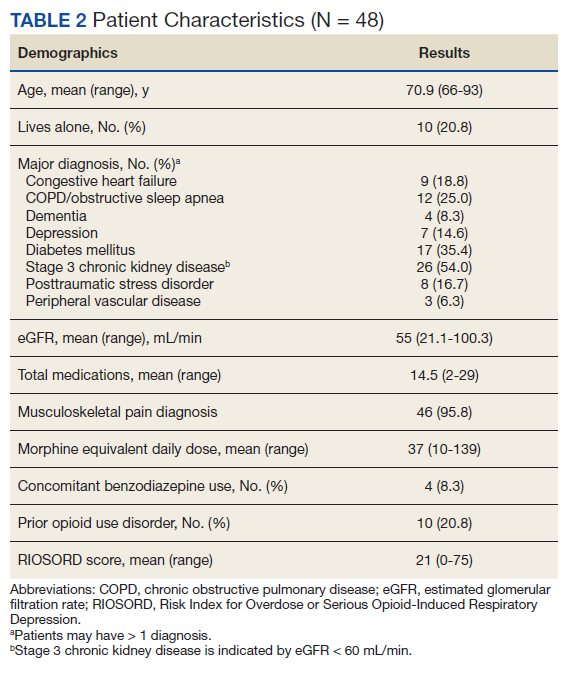
Results: The mean (range) age of patients was 70.4 (66-93) years. Many patients had comorbid conditions, such as diabetes mellitus (35%), congestive heart failure (18.6%), and dementia (8.3%). More than half had an estimated glomerular filtration rates (eGFR) < 60 mL/min, indicating at least stage 3 chronic kidney disease, 41.7% used mental health services (41.7%), and 20.8% had a history of opioid use disorder. Most indications for chronic pain were for musculoskeletal pain (95.8%). The mean (range) morphine equivalent daily dose was 37 mg (10-109). More than half had been seen in the emergency department, and 20.8% had been hospitalized in the previous year for an opioid-related hospitalization, and 3% had expired. Over the year, dose reductions of benzodiazepines or narcotics was performed for 12.5% of patients, accidental overdoses occurred in 4.2%, and positive urine drug screens (UDSs) for cocaine and cannabinoid/tetrahydrocannabinol occurred in 10.4%. One patient was terminated from the program for multiple positive UDSs.
Conclusions: Guideline-based patient-centered medical home management of patients with chronic pain who were treated with opioids can be an effective model contributing to the health and well-being of older patients. Complex older patients on chronic opioid treatment are best managed by an interdisciplinary team.
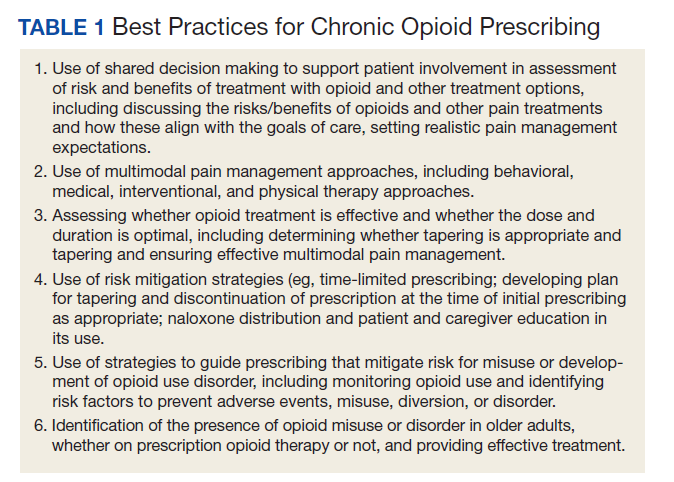
Best practices for prescription opioids for chronic pain follow the US Department of Health and Human Services Interagency Task Force pain management recommendations.4 These include: (1) Effective pain evaluation and management, including diagnostic evaluation and indicated referrals; (2) appropriately prescribed opioids when indicated; and (3) active management of opioid users to prevent AEs and misuse. Strategies used in GeriPACT were adopted from the pain management task force and designed to address needs and challenges associated with responsible chronic opioid prescribing (Table 1).
All 48 patients who were prescribed chronic opioid therapy received routine primary care at GeriPACT. A data tracking sheet was maintained from July 1, 2019 to June 30, 2020. Patients were presented for interdisciplinary collaboration and management at weekly GeriPACT where applicable continuous improvement processes were incorporated. Patients were seen every 3 to 6 months and offered dose reduction and alternative therapies at those times. All patients initiated monthly calls for medication refills and were monitored with an initial opioid contract and quarterly unannounced urine drug screens (UDSs) as well as a quarterly review of the prescription drug monitoring database (PDMD). Additionally, all patients received an Opioid Risk Tool assessment (scale 0-26; high risk ≥ 8) and a Risk Index for Overdose or Serious Opioid-Induced Respiratory Depression (RIOSORD) Score (scale 0-115).9,10 Patients with RIOSORD scores ≥ 25 (14% risk of opioid induced respiratory depression) were issued naloxone kits.
All VA patients additionally receive a risk stratification, the clinical assessment of need (CAN) score, which is a clinical predictor of hospitalization and death developed for VA populations.11 This methodology extracts predictors from 6 categories: social demographics, medical conditions, vital signs, prior year use of health services, medications, and laboratory tests and constructs logistic regression models to predict outcomes. CAN scores are on a 99-point scale, with higher scores corresponding to an increased probability of future health care events.
Our overall study was designed to meet standards for quality improvement reporting excellence (SQUIRE) criteria, and this report meets the quality improvement minimum quality criteria set (QI-MQCS) domains for reporting quality improvement work.12,13 The TVHS Institutional Review Board determined this study to be a quality improvement initiative.
Results
Chronic opioid patients comprised 6.4% of the GeriPACT population. These patients had many comorbidities, including diabetes mellitus (35%), pulmonary disease (25%), congestive heart failure (18.8%), and dementia (8%). There were 54% with estimated glomerular filtration rates (eGFR) < 60 mL/min, indicating at least stage 3 chronic kidney disease (Table 2). Patients had an average RIOSORD Score of 21 and a 14% risk of opioid induced respiratory depression, and 20% received mental health services.
The mean CAN score was 83.1, suggesting a 1-year risk of 20% for a major AE and 5% mortality risk. Many patients with chronic opioid use were transferred to GeriPACT from primary care due to presence of complex medical issues in addition to need for chronic pain management. In this population, 8% were coprescribed benzodiazepines and opioids. Consults were obtained from interventional pain for 37.5% of patients and palliative care for 27% of patients, the majority for goals of care related to chronic illness and advance directive discussions, and in 1 patient for pain and symptom management. The majority of patients (81%) had advance care planning documents or discussions documented in the electronic health record, and 87.5% of patients received home and community-based support in addition to GeriPACT care.
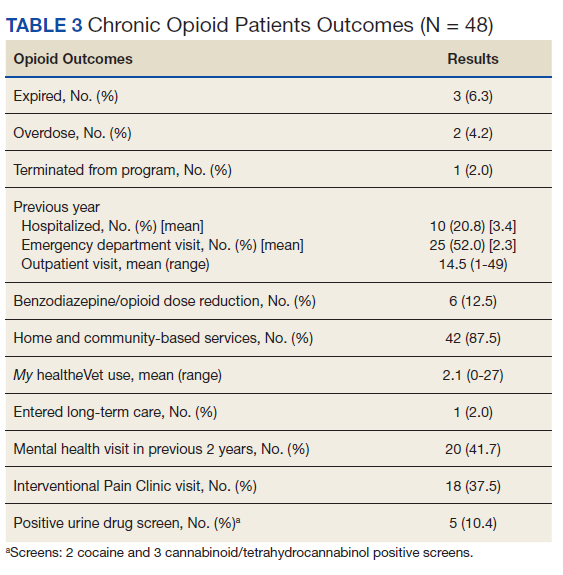
My healtheVet patient portal secure messaging was used a mean 2.1 times per patient (range 0-27) to maintain contact with GeriPACT providers and patients had a mean 14.5 outpatient visits yearly (range, 1-49) in addition to monthly clinic contact for opioid prescription refills (Table 3). One patient entered long-term care. Three patients expired due to congestive heart failure, sepsis, and complications following a hip fracture. Of the patients who expired, all had advance directives or hospice care involvement. The VA STORM risk tool identifies the highest risk patients: suicide risk, current opioid or substance use disorder, suicide attempt or overdose during the past year, and potential for opioid-related respiratory depression on the RIOSORD scale. None of the panel patients met high-risk criteria on the Opioid Risk Tool assessment or were identified on the facility’s highest risk category by the STORM risk tool.