Assessment of Consolidated Mail Outpatient Pharmacy Utilization in the Indian Health Service





Background: The Indian Health Service (IHS) has an agreement with the US Department of Veterans Affairs (VA) that allows IHS to use the VA Consolidated Mail Outpatient Pharmacy (CMOP) to send prescriptions to IHS patients. However, there is high variability among IHS facilities in the use of CMOP. Furthermore, there is no available resource that summarizes the relative positives/negatives, challenges/opportunities, and strengths/weaknesses of implementing CMOP.
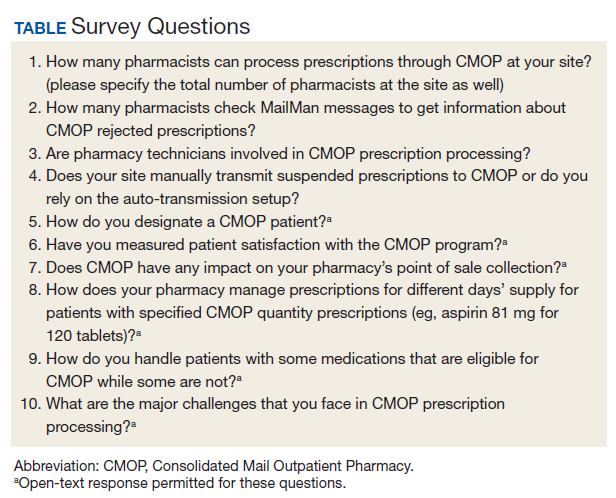
Methods: A 10-item questionnaire was developed to collect information on various aspects of prescription processing through CMOP. The questionnaire was distributed among the primary CMOP contacts of IHS facilities between December 2018 and January 2019.
Results: The CMOP contacts at 44 of 94 (47%) IHS sites responded to the survey. Of the 347 respondents, 310 (89%) pharmacists were trained in CMOP prescription processing. To get information about CMOP rejections, 53% (185/347) of pharmacists check electronic messages. Twelve (27%) sites utilize technicians in some capacity in the CMOP process. Of the 16 facilities that require patients to request prescriptions to be mailed for each refill request, 8 (50%) do not use any method to designate a CMOP patient. Three sites (7%) have measured patient satisfaction with the CMOP program. Thirteen sites (31%) reported that they are losing insurance reimbursements by using CMOP. The decrease in insurance reimbursements, lengthy prescription processing time, and medication backorders are the most common challenges shared by respondents.
Conclusions: CMOP presents unique challenges to pharmacy workflow but provides many benefits that local pharmacy mail-out programs usually do not possess, such as the ability to mail refrigerated items. Furthermore, it is likely that local programs that utilize mail delivery will increase pharmacy workload. However, there is a lack of objective data to assess the net effect of CMOP on patients. Nevertheless, the successful implementation of CMOP can lead to reduced pharmacy workload while increasing access to care for patients with transportation issues.
Methods
A questionnaire encompassing various aspects of CMOP prescription processing was developed and distributed to the primary CMOP contacts for IHS facilities. The questionnaire was first distributed by e-mail on December 19, 2018. It was e-mailed for a second time on January 16, 2019, and the questionnaire was open for responses until the end of January 2019 (Table).
Results
Forty-four of 94 CMOP-enrolled IHS sites responded to the questionnaire. Most sites train the majority of their pharmacists in CMOP prescription processing. Overall, 310 of 347 pharmacists (89%) in these 44 IHS sites can process prescriptions through CMOP. Thirty-one sites have all their pharmacists trained in CMOP prescription processing. Only 1 facility had less than half (2 of 17 pharmacists) of its pharmacists trained in CMOP prescription processing. More than half the total number of pharmacists, 185 out of 347 (53%), check electronic messages via Resource and Patient Management System (RPMS) MailMan to get information about prescriptions rejected by CMOP. Twenty sites have all their pharmacists check messages about CMOP rejections. However, 2 facilities reported that they do not check the rejection messages at all. Twenty-six of the 44 responding sites (59%) transmit prescriptions to CMOP manually in the electronic system. The rest (18 of 44) rely on the auto-transmission (AT) setup to transmit the CMOP-suspended prescriptions at specified times of the day.
Half the sites (8 of 16) that rely on patients asking for prescriptions to be mailed at the time of refill request do not use any method to designate a CMOP patient. Twenty-four sites use the narrative field on the patient’s profile in RPMS, the health information system used by most IHS facilities, to designate CMOP patients. Eighteen sites use pop-up messages on ScriptPro, a pharmacy automation system, as a designation method. Most of the sites (12 of 15) that use both RPMS and ScriptPro designation methods do not require patients to ask for prescriptions to be mailed at the time of refill request; prescriptions for these patients are routed through CMOP unless patients request otherwise. Only 3 of 44 sites use both methods and rely on patients asking for prescriptions to be mailed at the time of refill request. Some other reported designation methods were using the electronic health record (EHR) posting box, keeping a manual list of CMOP patients, and solely utilizing the Prescription Mail Delivery field in RPMS. Three sites also noted that they keep manual lists to auto-refill prescriptions through CMOP.
Thirty sites (68%) reported that they process every prescription through CMOP even if the patient had prescriptions with specified CMOP quantities. Only 8 sites (18%) said that they used the local mail-out program to keep the same days’ supply for all medication orders. For patients with CMOP-ineligible prescriptions, 34 of the 44 sites (77%) process the eligible prescriptions through CMOP and refill the rest of the prescriptions locally. Six sites (14%) process all medication orders locally for patients with any CMOP-ineligible prescriptions.
Only 12 of 44 sites (27%) involve pharmacy technicians in CMOP prescription processing. Five sites have technicians process prescription refills through CMOP. Two of these sites mentioned the strategy of technicians suspending the prescriptions to be sent to CMOP on the refill due date. Other technician roles included tracking CMOP packages, checking electronic messages for CMOP rejections, and signing up patients for CMOP.
Only 3 of the 44 sites (7%) have measured patient satisfaction with the CMOP program. One of these 3 sites reported that the overall satisfaction was high with CMOP. This site administered the survey to patients who came to the clinic for appointments. The second facility called patients and asked for their feedback. The third site conducted the survey by using student pharmacists. Two sites reported that they use the survey results from the CMOP-conducted patient satisfaction surveys, although they have not measured patient satisfaction at their specific facilities.
Most sites have not assessed CMOP’s impact on their insurance (point of sale) collections. However, 13 sites (30%) reported that they believe they are losing on collections by utilizing CMOP. The use of repackaged products by CMOP, which are usually nonreimbursable, is an issue that was mentioned multiple times. In contrast, 2 sites mentioned that CMOP has led to increased insurance collections for their facilities.