The Relationship Between Male Patients’ Antihypertensive Medication Beliefs and Erectile Function





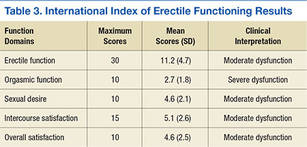
All of the respondents self-reported sexual dysfunction as indicated by the mean scores on the 5 domains of the IIEF (Table 3). Moreover, the vast majority of the total scores on the 5 domains fell within the moderate-to-severe dysfunction levels (Table 4).
BMQ Scores
The mean BMQ specific-necessity score was 16.7 (Table 5). More than half the respondents agreed or strongly agreed with 4 of the 5 statements regarding the necessity of their medications; the exception was “My life would be impossible without my medicines” (29.8%). The statement that generated the highest percentage of agreement was “My medicines protect me from becoming worse” (72.3%) (Table 6).
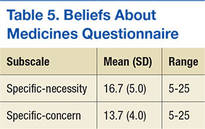
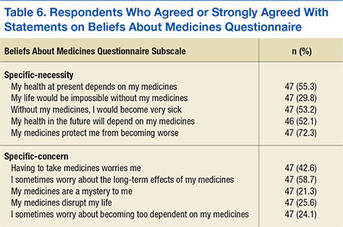
The mean BMQ specific-concern score was 13.7. Less than one-fourth of the respondents agreed or strongly agreed with 3 statements (of 4) regarding medication concerns: “My medicine is a mystery to me” (21.3%), “I sometimes worry about becoming too dependent on my medicine” (24.1%), and “My medicines disrupt my life” (25.6%). Regarding the fourth statement, “I sometimes worry about the long-term effects of my medicines,” 58.7% agreed or strongly agreed.
Spearman correlation analyses were performed to examine the relationships between BMQ specific-necessity, BMQ specific-concern, and the 5 IIEF sexual functioning domains. No statistically significant relationships were detected.
Time With Hypertension Diagnosis
The study also evaluated the results based on length of time the men had a hypertension diagnosis (≤ 10 years vs ≥ 11 years). An independent t test was used to compare mean BMQ specific-necessity and specific-concern scores. Crosstabs was used to compare length of time with diagnosis and the 5 IIEF domains. Mean specific-necessity score was 18.1 for the 20 respondents with a diagnosis of ≥ 11 years and 15.0 for the 22 respondents with a diagnosis of ≤ 10 years; this difference was statistically significant (P = .048). In addition, mean specific-concern score was 14.7 for respondents with a diagnosis of ≥ 11 years and 12.4 for those with a diagnosis of ≤ 10 years; this difference was not statistically significant but was trending in that direction (P = .076).
Length of time with a hypertension diagnosis did not necessarily relate to sexual function or satisfaction. Moderate-to-severe dysfunction in sexual desire was reported by 42% of the respondents with a diagnosis of ≥ 11 years compared with 57% of those with a diagnosis of ≤ 10 years. The same was found for overall satisfaction.
Discussion
Men with chronic health conditions, such as hypertension, are often prescribed medications that interfere with their sexual functioning.5 Patients who do not understand the importance of medication adherence in treating long-term chronic health conditions may discontinue taking these medications to improve their sexual functioning.5 Some men overestimate the control they have over chronic health conditions; others underestimate their control.
With a better understanding of men’s perceived ability to control chronic hypertension, practitioners can begin to provide appropriate educational interventions. These interventions must inform patients about the role of medication adherence in maintaining and enhancing sexual functioning and must impart a greater sense of control and empowerment over their condition, thereby increasing the likelihood of medication adherence.
To the authors’ knowledge, this is the first study to examine the potential associations of medication beliefs (using the BMQ) and erectile function in men with hypertension. There was no association between any of the demographic variables of age, race, marital status, and education, with respondents’ medication beliefs or erectile function. The IIEF domain that had the highest level of severe and moderate dysfunction combined was orgasmic function (n = 36; 80%), which suggests that antihypertensive medication may interfere with orgasmic function because achieving an orgasm is a physiologic process. This is consistent with the findings of Hellstrom and colleagues—that the vast majority of ED is related to orgasmic factors.6 Although 80% of respondents reported either moderate or severe dysfunction in this area, only 53% (n = 24) reported moderate or severe dysfunction in overall satisfaction. This might suggest that men taking antihypertensive medication, and their partners, have learned other methods or strategies for achieving sexual satisfaction.
The BMQ specific-necessity and specific-concern results offer insight into how men with hypertension view the need for antihypertensive medication. Mean (SD) specific-necessity score was 16.7 (5); the maximum was 25. Although no other studies have investigated men’s beliefs about antihypertensive medications, studies of other chronic illnesses have measured beliefs about the medications used in treatment. For example, Neame and Hammond reported a mean specific-necessity score of 19.9 and a mean specific-concern score of 15.9 in a sample of 108 men with arthritis.7 Of the respondents, 74.3% agreed or strongly agreed that their arthritis medication was necessary for health. However, 47.4% were concerned about potential adverse effects. Lennerling and Forsberg conducted a cross-sectional study of 250 renal transplant recipients.8 Respondents reported a mean specific-necessity score of 23 and a median specific-concern score of 11. In addition, length of time with hypertension diagnosis affected specific-necessity and specific-concern scores. For example, men with a hypertension diagnosis for 10 or fewer years had higher scores on both of these BMQ subscales.