Preventing and treating acute gout attacks across the clinical spectrum: A roundtable discussion





THE ROLE OF COMORBIDITIES IN THERAPY CHOICE
Chronic kidney disease
Dr. Mandell: Let’s get more specific about comorbidities and therapy choice, starting with chronic kidney disease. What’s the threshold at which renal compromise starts to influence your choice of therapy for an acute attack of gout?
Dr. Sundy: I have a very low threshold for avoiding NSAIDs in that setting, mainly because when I want to use NSAIDs, I want to use them at a very high dose, and even short-term use of high-dose NSAIDs can reduce creatinine clearance. So I would certainly avoid NSAIDs when the patient’s creatinine clearance is less than 60 mL/min, and I’d be even more cautious if the patient had underlying hypertension or congestive heart failure.
Dr. Mandell: So even with the reversibility of almost all of the NSAIDs’ renal effects, you tend to stay away from them in that setting?
Dr. Sundy: Yes.
Dr. Edwards: I’m less guided by a single creatinine clearance level. I tend to look at patients in light of the 20% to 25% reduction in the glomerular filtration rate (GFR) that most NSAIDs will cause, even when used acutely. Though the NSAID effect is reversible, if that GFR reduction is going to make a difference to other compensated systems, primarily the heart, then the NSAID should be avoided.
Dr. Simkin: It’s my understanding that plasma flow to the kidney becomes prostaglandin dependent with renal insufficiency, and when we use antiprostaglandin agents we get into trouble on a mechanistic level. I’m not sure of the exact point at which that occurs, but I think we all recognize that serum creatinine is a fairly weak indicator of which patients have some limitation.
Dr. Mandell: So we agree on the need to be very cautious with the use of NSAIDs, recognizing that in the acute setting there is reversibly depressed renal blood flow from NSAIDs. The decreased blood flow will get better, but there’s the issue of what happens during fluid retention when there is coexistent congestive heart failure, diabetes, and chronic kidney disease—you may also occasionally bump up the potassium level. In general, most rheumatologists shy away from selective or nonselective NSAIDs in the setting of chronic kidney disease. Is that consistent with the use you see in the hospital, Jim?
Dr. Pile: It is. I would add that if patients are on certain other medications—especially angiotensin-converting enzyme inhibitors, angiotensin receptor blockers, or beta-blockers—there may be additive negative effects because of the potential for hyperkalemia if an NSAID were added to the mix.
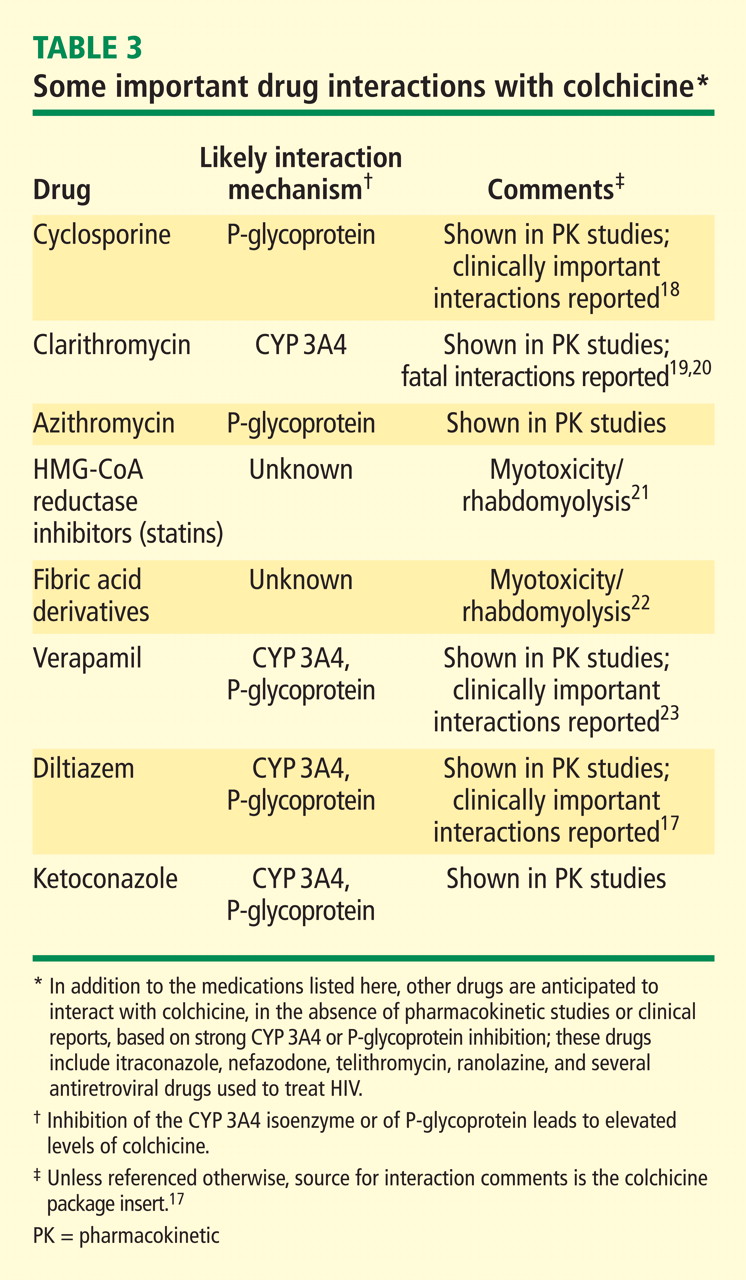
Dr. Mandell: I would add to that list of concerning medications aminoglycosides, cyclosporine, and other nephrotoxic agents.
Diabetes
Dr. Mandell: What about diabetes? How does a patient’s diabetes enter into your choice of acute gout therapy in the outpatient and inpatient settings?
Dr. Edwards: Diabetes is especially problematic because it significantly affects two of our treatment choices—steroids and NSAIDs. The steroid doses needed to effectively treat an acute gout attack have a pretty profound effect on glucose levels in diabetic patients. That’s always of concern to me, and it’s certainly of concern to my patients with diabetes who are vigilant about monitoring their glucose levels, which may spike from 130 or 140 mg/dL to values in the high 200s. These elevations will last for the 7 to 10 days of treatment, and the longterm adverse effects of that period of hyperglycemia are not clear. If we put these patients on short courses of corticosteroids, perhaps we should be treating their diabetes more aggressively during that period, but I don’t think we have a history of doing that.
Dr. Pile: It’s very difficult to do in the short term. That’s especially the case with the diabetic patients I see as a hospitalist at a safety-net hospital. Many of my patients don’t have good glucose control at baseline: their levels of 250 mg/dL may go to 400 mg/dL or higher with acute corticosteroid therapy, so that’s clearly a problem.
Dr. Mandell: I try to avoid giving corticosteroids in the outpatient setting to a diabetic patient who is being maintained on oral hypoglycemic medications, particularly if efforts are being made to avoid more aggressive diabetes therapy. Steroids may be an option, though, for a patient who is on insulin, uses a pump, and is very comfortable measuring and managing his or her glucose at home. In the hospital setting, I’m more comfortable using corticosteroids in diabetics because I have much better control over their glucose; I can just increase the basal and premeal coverage.
Dr. Pile: I agree. With vigilance I can control almost anyone’s blood sugar in the hospital, but when patients leave the hospital on steroids, it becomes much more problematic.
Dr. Mandell: Right. You don’t know what’s going to happen when they go out and liberalize their diet on top of the steroids, because often it’s the postprandial surge that’s exacerbated by steroids.
Dr. Sundy: It can be very helpful to know at baseline what a patient’s spot blood sugar is before using a steroid, just as it’s important to know what the creatinine is before considering an NSAID. In the setting of an acute flare, the patient might already be quite hyperglycemic, and many of these patients probably don’t have the tools to manage this at home, so careful follow-up—coming back the next day for at least a blood sugar check—is critical to the proper care of these patients.
Dr. Mandell: When we talk about steroids we tend to think mostly about prednisone, but Peter mentioned injectable steroid. What about injectable adrenocorticotropic hormone (ACTH), which goes in and out of vogue as an agent to treat acute gout? What is your experience with using ACTH injections, specifically related to the issues of diabetes and heart failure?
Dr. Edwards: Before it got reformulated about 3 or 4 years ago and its price went way up, injectable ACTH was my drug of choice for treating acute gout. I had hardly any failures on it over the 10 to 15 years when it was my main means of treating acute gout. I would typically use 80 IU of ACTH gel, given subcutaneously, and the response within 12 hours was quite dramatic. About one in four patients would require a second injection at that 12-hour point, but almost everyone was symptomfree at 24 hours. This response was seen even in patients who were on fairly high-dose chronic steroids already, such as transplant patients.
This suggested that a mechanism other than just adrenocortical stimulation explained the benefit from ACTH. In fact, a lot of data have emerged suggesting that ACTH has a specific effect that is not related to adrenocortical stimulation.
Ten years ago an injection of ACTH gel would cost about $3 or $4, whereas today it costs $2,000 or more.29 I don’t think it’s justifiable at that cost.
Dr. Mandell: There’s also the issue of fluid retention with ACTH, and the higher doses, which seem to be more effective, are more likely to exacerbate congestive heart failure, which has to be a concern if you go this route.
Coronary artery disease
Dr. Mandell: Atherosclerosis, diabetes, and chronic kidney disease are increasingly recognized in the gout population, and coronary artery disease links with all of those. Does the presence of coronary artery disease enter into your choice of agents for a patient with an acute attack of gout?
Dr. Edwards: It doesn’t have as big an impact as diabetes does. To me, the priority in this setting is resolving the acute attack as quickly as possible, as I’ve seen my share of patients for whom the acute gout attack has been so painful and stressful that they’ve developed angina at the same time. So I might use steroids in patients with coronary disease because I’ll want to go with what’s likely to be most efficacious for quick resolution of the attack even though steroids may increase glucose and blood pressure and thus raise fluid retention as an issue.
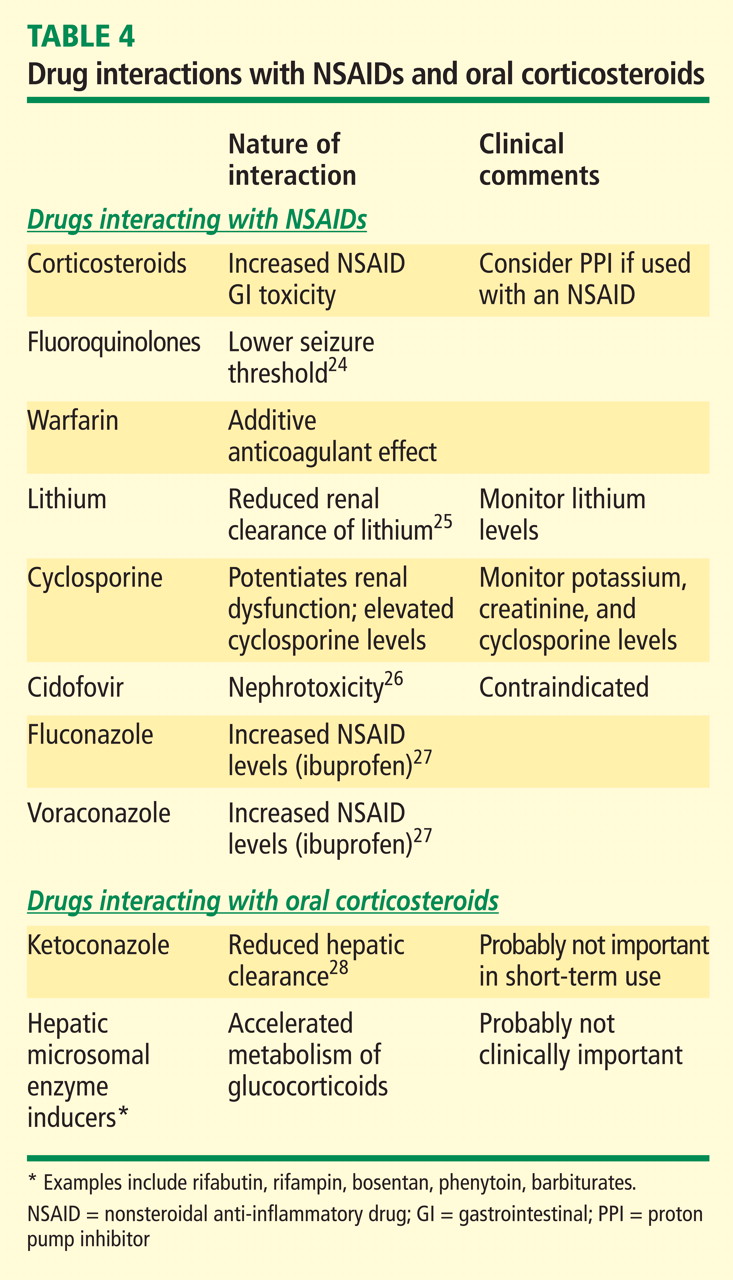
Dr. Mandell: The presence of coronary disease implies the use of low-dose aspirin therapy. Despite the slight elevation in serum urate from low-dose aspirin, I recommend that my gout patients continue this for coronary protection. But even low-dose aspirin raises concerns of GI safety and even possible drug interactions with ibuprofen that could reduce the aspirin’s efficacy. Does this lessen your tendency to reach for an NSAID in these patients?
Dr. Edwards: I think the issue of cardiovascular safety and NSAIDs is still up in the air. The data that came out around the time the selective COX-2 inhibitors were released made us all think again about the role of prostaglandins and coronary blood flow and how blocking prostaglandins might have some bad effects. I don’t often use NSAIDs in patients with significant heart disease, simply because they don’t act fast enough to get patients through the attack quickly and I worry about the sodium retention and other problems putting stress on the heart.
Dr. Sundy: While coronary disease doesn’t create the acute dilemmas that diabetes does, it is a consideration in my therapy choice, and I generally avoid using NSAIDs.
Dr. Mandell: It is important to remember the additive gastric toxicity effect from low-dose aspirin and NSAIDs.