
Androgens in women: To replace or not?






Androgen therapy can improve sexual desire and response—here’s how
IN THIS ARTICLE
TABLE 2
Testosterone therapies available now—or in the pipeline
| Oral |
|
| Intramuscular |
|
| Subcutaneous (implant) |
|
| Transdermal |
|
| Other |
|
How long until relief?
It is clear from a number of studies13,14 that estrogen plus methyltestosterone oral replacement improves sexual desire in women after 12 to 16 weeks, and that this improvement is based on an increase in bioavailable testosterone. A testosterone patch under development delivers 300 μg per day. When used with conjugated equine estrogens, this patch has been shown to increase bioavailable testosterone in women without ovaries who have very low androgen levels.3
In a 2005 study,15 more than 500 women with hypoactive sexual desire who had undergone a total abdominal hysterectomy–bilateral salpingo-oophorectomy were randomized to placebo or a testosterone patch that delivered 300 μg per day for 24 weeks. Not only did serum testosterone levels increase, but satisfying sexual activity and the numbers of sexual interactions and orgasms increased (FIGURE 3). Side effects of therapy included increased facial hair and acne, but there was no increase in serious adverse effects, and no increase in withdrawal from the study because of side effects. Unfortunately, this patch is in development and unavailable commercially in the United States.
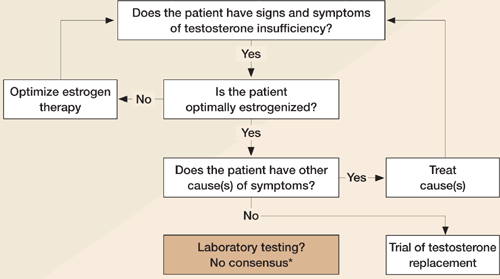
FIGURE 3
Assessing testosterone status in women
Adapted from Braunstein GD20
*Bachmann G, et al11
Watch for side effects, and follow closely
Testosterone therapy is most appropriate for women who have undergone surgical menopause and for postmenopausal women who are dissatisfied with estrogen therapy because of symptoms such as decreased libido and a diminished sense of well-being, including headaches and fatigue. Side effects of testosterone therapy include hirsutism, acne, alopecia, worsening lipoproteins, and, in the case of methyltestosterone, the possibility of liver toxicity, so women receiving testosterone should be followed frequently and carefully to detect any of these effects.
Androgen insufficiency in a nutshell
Androgens in women engender a general sense of well-being, which includes elevated energy and mood and increased libido. It is appropriate to consider androgen replacement using oral methyltestosterone, androgen implants, or transdermal androgen gels in women with a clinical diagnosis of androgen insufficiency.
Before initiating androgen therapy, however, it is important to measure total androgen level and assess clinical symptoms. Also, monitor the incidence of side effects to ensure that the patient does not exceed normal female androgen levels. It is hoped that additional forms of androgen replacement for women will become available in the near future.
The role of testosterone therapy in postmenopausal women: position statement of The North American Menopause Society. Menopause. 2005;12:497–511.
In 2005, the North American Menopause Society issued a comprehensive position statement on the role of testosterone therapy in postmenopausal women. Its purpose was to offer recommendations based on reliable evidence, and it reflects a thorough analysis of the data to date. Note that its findings, highlighted below, pertain to postmenopausal women only.
1. Endogenous testosterone levels have no clear link to sexual function
No definitive studies have established a relationship between endogenous testosterone levels and sexual function, and observational data have been mixed. Because of this lack of clarity, we do not have specific total or free testosterone values that indicate clinical testosterone deficiency.
Exogenous testosterone is a different story. Randomized controlled trials have demonstrated greater sexual desire and sexual responsiveness and more frequent sexual activity when exogenous testosterone is given. Almost all trials involved testosterone combined with estrogen or estrogen–progestogen therapy. The only trial that included a testosterone-alone arm found that testosterone added to estrogen therapy or given alone increased sexual desire, arousal, and frequency of sexual fantasies, compared with placebo or estrogen alone.14
2. Use the free testosterone index to determine testosterone bioavailability
Only 1% to 2% of circulating testosterone is free or bioavailable. The remainder binds tightly to sex hormone-binding globulin (SHBG, about 65%) or loosely to albumin (~30%). Because oral estrogen therapy increases SHBG levels, it lowers unbound testosterone. Conversely, obesity and hypothyroidism depress SHBG levels and increase free testosterone.
The simplest method to determine the amount of bioavailable testosterone is to measure total testosterone and SHBG, dividing total testosterone (ng/dL) by SHBG (nmol/L). Multiply this figure by 3.47 to obtain the free testosterone index. If the total testosterone value is reported in nmol/L, the multiplication factor is 100.
During the menopausal transition, free testosterone concentrations appear to remain fairly constant or increase slightly, probably because SHBG declines as ovarian estrogen production diminishes. One small study found little difference in total testosterone between younger premenopausal women (age 19–37 years) and older women (age 43–47), although the older age group lacked the midcycle rise in free testosterone and androstenedione.16
3. Causes of androgen insufficiency: Chronic illness, age, and oophorectomy, to name a few
Bilateral oophorectomy can lower testosterone levels by as much as 50%. Other contributors include increasing age, hypothalamic–pituitary–adrenal insufficiency, systemic glucocorticoids, hyperthyroidism and excessive thyroid medication, and chronic illness such as depression and advanced cancer. Both endogenous and exogenous estrogens lower testosterone levels by raising SHBG.
4. Sexual dysfunction is the only indication
Thus far, we lack sufficient data to justify use of testosterone for any other indication, including preserving bone mineral density, reducing hot flashes, and improving the patient’s overall sense of well-being.
5. A comprehensive clinical exam is mandatory
This includes a psychosexual and psychosocial history; a thorough medical history, including use of prescription and other drugs (such as selective serotonin reuptake inhibitors, which can reduce sexual desire); and a physical exam. It may also be appropriate to measure thyroid-stimulating hormone and prolactin and get a complete blood cell count. Consider the effects of other physical, psychological, and emotional complaints on sexual function, and ask about the relationship itself.
A study from Australia17 concluded that a postmenopausal woman’s previous level of sexual function, her feelings toward her partner, any change in partner status, and estradiol levels have the greatest influence on her sexual interest, arousal, and enjoyment. Declining levels of estradiol at menopause have a smaller impact than these psychological factors.
6. Non-oral forms of testosterone are preferred
To avoid the first-pass hepatic effects of oral administration, prescribe transdermal patches and topical gels and creams whenever possible, rather than oral testosterone.
Oral testosterone in combination with oral estrogen reduces high-density lipoprotein cholesterol and triglycerides in postmenopausal women, but non-oral testosterone has no significant effect on these parameters.
Extended use of high doses of oral testosterone can cause liver dysfunction in women.
7. Impact on fracture risk is unclear
Adding testosterone to estrogen therapy increases bone mineral density or reduces bone turnover, but no randomized trial has reported its effects on fracture risk in postmenopausal women.
8. No testosterone product is FDA-approved for sexual dysfunction in women
However, a few testosterone-containing prescription products are approved for use by women and men; some of these are used “off-label” to treat diminished sexual desire in women.
Be wary of custom-compounded prescription formulations because they do not undergo the same rigorous quality control as FDA-approved products.
A number of testosterone products are under development specifically for female sexual desire disorders, including an oral product, a cream, gels, a patch, a spray, and a vaginal ring.
9. Avoid testosterone in cancer and in heart and liver disease
Testosterone therapy is contraindicated in patients who have cancer of the breast or uterus, or cardiovascular or liver disease.
10. As with estrogen, use the lowest dosage for the shortest time possible
Once therapy meets treatment goals, it should be curtailed, if possible. And the dose should be kept as low as possible.
Most trials of testosterone therapy lasted 6 months or less, so we lack long-term data on safety and efficacy.
11. Supraphysiologic levels can cause adverse effects, some of them permanent
Risks include lowering of the voice (which may be permanent), enlargement of the clitoris, excess body hair, erythrocytosis, edema, and liver dysfunction. Psychological effects are also possible.
