Sonography of ovarian masses: 9 key questions to guide clinical evaluation






Hallmark characteristics of benign and malignant lesions help point to the need for surgery. An expert sonologist details morphologic criteria that assist in diagnosis.
For example, a recent hemorrhagic cyst may result in an enlarged ovary with mixed echogenicity. Over 6 weeks the liquefaction of the clot within the cyst will result in either resolution of the mass or a markedly different sonographic appearance.
Other studies
Ovarian Doppler. Because of the many types of ovarian masses, sonographic morphology is usually not pathognomic and—when used alone—results in a high false-positive rate in the diagnosis of malignancy. The role of color and pulse Doppler is to reduce these false-positives. Note, however, that the positive predictive value of gray scale and color Doppler is lower in premenopausal patients than postmenopausal women because of the higher prevalence of malignancy in the latter group.
Although initial color Doppler studies of ovarian masses suggested that clinicians could use a cut-off resistance index (FIGURE 7) or pulsatility index to satisfactorily discriminate between benign and malignant lesions,25 subsequent studies demonstrated considerable overlap in the values obtained.26 As a result, evaluation of vessel distribution and architecture has taken on additional importance (FIGURE 8).
- Findings suggestive of malignancy. Malignant tumors characteristically contain dilated, saccular, and randomly dispersed vessels.27 Centrally located flow, flow along septations, and flow within papillary excrescences also suggest malignancy.
- Findings suggesting a benign mass. Peripheral flow is more consistent with a benign neoplasm. Hemorrhage in a mass is highly suggestive of a benign mass or cyst.28
Morphology scores. Almost monthly a new morphology scoring system is published that attempts to substitute objective criteria and measurements for the subjective assessment of an ovarian mass. Most morphologic scoring systems include the parameters reviewed thus far, and some include menopausal status and CA-125 values. Sensitivities and specificities as high as 95% have been reported.29
Inevitably, when these scoring systems are validated externally, both the sensitivity and specificity fall. Currently, the proposed models perform no better than an experienced clinician using the patient’s history, sonographic findings, and CA-125 measurement.30
Three-dimensional sonography. Three-dimensional power imaging may enable visualization of malignant vessel abnormalities (ie, arteriovenous shunts, tumor lakes, etc). It also may improve the evaluation of tumor architecture and tumor invasion through the ovarian capsule. To date, however, 3-dimensional imaging has not been shown to significantly affect the morphology score assigned by 2-dimensional imaging.31
Dr. Hill reports no financial relationship with any companies whose products are mentioned in this article
FIGURE 7 Malignancy

A 55-year-old patient with an 11-cm right ovarian malignancy. A) A 4.5-cm echogenic foucs within the primary systic mass.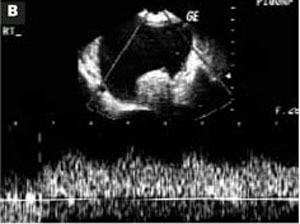
B) Low resistance index (0.297) in a peripheral vessel.
FIGURE 8 Power Doppler

Power Doppler of abnormal vessels within an ovarian carcinoma.