Care Transitions Program for High-Risk Frail Older Adults is Most Beneficial for Patients with Cognitive Impairment





BACKGROUND: Although posthospitalization care transitions programs (CTP) are highly diverse, their overall program thoroughness is most predictive of their success.
OBJECTIVE: To identify components of a successful homebased CTP and patient characteristics that are most predictive of reduced 30-day readmissions.
DESIGN: Retrospective cohort.
PATIENTS: A total of 315 community-dwelling, hospitalized, older adults (≥60 years) at high risk for readmission (Elder Risk Assessment score ≥16), discharged home over the period of January 1, 2011 to June 30, 2013.
SETTING: Midwest primary care practice in an integrated health system.
INTERVENTION: Enrollment in a CTP during acute hospitalization.
MEASUREMENTS: The primary outcome was all-cause readmission within 30 days of the first CTP evaluation. Logistic regression was used to examine independent variables, including patient demographics, comorbidities, number of medications, completion, and timing of program fidelity measures, and prior utilization of healthcare.
RESULTS: The overall 30-day readmission rate was 17.1%. The intensity of follow-up varied among patients, with 17.1% and 50.8% of the patients requiring one and ≥3 home visits, respectively, within 30 days. More than half (54.6%) required visits beyond 30 days. Compared with patients who were not readmitted, readmitted patients were less likely to exhibit cognitive impairment (29.6% vs 46.0%; P = .03) and were more likely to have high medication use (59.3% vs 44.4%; P = .047), more emergency department (ED; 0.8 vs 0.4; P = .03) and primary care visits (4.0 vs 3.0; P = .018), and longer cumulative time in the hospital (4.6 vs 2.5 days; P = .03) within 180 days of the index hospitalization. Multivariable analysis indicated that only cognitive impairment and previous ED visits were important predictors of readmission.
CONCLUSIONS: No single CTP component reliably predicted reduced readmission risk. Patients with cognitive impairment and polypharmacy derived the most benefit from the program.
© 2019 Society of Hospital Medicine
The present study met our objective of identifying individual patient factors that are predictive of the success of our CTP. Cognitively impaired patients were less likely to be readmitted than cognitively intact patients. This finding is particularly important because patients with dementia constitute a subgroup that is at an increased risk of readmission after hospitalization29 and often suffer burdensome transitions at the end of life.30,31 High medication use and high number of visits to primary care and number of hospital days in the six months leading up to enrollment increase the likelihood of readmission and are plausible measures of disease severity or multi-morbidity that have been identified in previous studies.32,33 No one program intervention was found to be significantly associated with readmission. This result is consistent with prior works that demonstrated the need for multifaceted and intensive interventions to reduce readmission risk among highly complex and multimorbid patients.13,14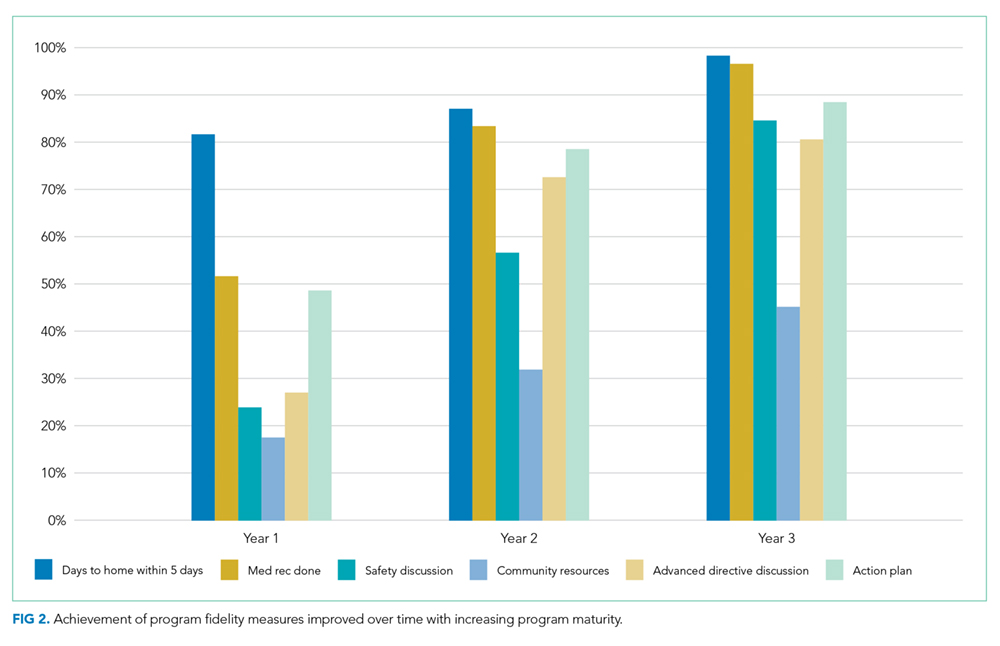
Our findings suggest that the provision of an alternative to stressful hospitalization to cognitively impaired patients and their caregivers may be an important benefit of care transitions programs. Having a trusted team to consult in acute situations may have enabled early intervention and crisis avoidance. Avoiding hospitalizations and ED visits may also have been in line with their goals of care.34,35 Given that program intensity varied on the basis of the discretion of the clinical team, patients with cognitive impairment and their caregivers may also have received more intensive support than cognitively intact patients.
In contrast to recent systematic reviews, our study did not find that advance directive discussion had significant effects on reductions in readmission.36,37 The lack of discussion surrounding the goals of care for patients with serious illnesses was also listed as one of four factors that are strongly associated with preventability in a national cohort of readmitted general medicine patients.38 The lack of power and incomplete documentation may have contributed to our null findings. Trust building must also occur before any meaningful discussion of the goals of care could be achieved, and follow-up time may have to be extended. Toward the end of this study, we developed an extension of our program for patients with limited life expectancy and conservative goals of care. In this extension, reductions in hospitalizations were observed among patients who had multiple goals of care discussions.28
Previous studies have shown that readmissions reduced with timely follow up among patients with heart failure.39 Our results showed no difference in readmission rate based on whether or not our patients were visited within five days from discharge, but we may have been underpowered to detect this difference. In addition, we may have missed readmissions that occurred before the enrollment visit.
The elements of the CTP were evidence based. Fidelity to program goals improved over time and reached high levels with program maturity. Only 12% of the patients received all program components at the first home visit. Patients that had all pillars addressed and documented showed a nonsignificant trend toward reduced readmission rates. NPs were given discretion as to how many visits were required to stabilize a patient and achieve program objectives. Heart failure management was driven by protocol with input from cardiology. Medication reconciliation and clinical assessment with action plan were prioritized at the first visit and thus allowed for the completion of other goals at a subsequent visit if time was insufficient. These decisions were deliberated at weekly physician-led multidisciplinary meetings. This variability allowed the team to meet chronic and urgent needs but further confounded the interpretation of our results. One possible way to interpret the lack of significant predictors of success is that through clinical assessment and flexibility, we were able to tailor our program to meet the needs of this complex multi-morbid population.
This study has important limitations. Given that it is a retrospective cohort study, we were unable to include patients who were enrolled but were either readmitted or dropped out before the first program visit. In addition, because of our study’s limited sample size and readmission rate, we had limited power to detect other potential predictor variables and test for confounding and interaction. While we included numerous variables in our analyses, we lacked information on mental health and the social determinants of health, which are known to influence readmission risk.40,41 Similarly, we lacked patient self-reported measures of health and information regarding caregiver support, which are important.42,43 Several of our predictive measures (cognitive impairment, mobility limitations, and program objective completion) were dependent on supplementing billing codes with heterogeneous data abstracted from usual clinical care as opposed to standardized research protocols. Neither method is completely accurate, nor can the combination of the two be assumed to be without inaccuracies. Failure to adequately document the clinical interventions performed by the clinical team is possibly a major confounder as evidenced by the considerable lack of agreement by our trained abstractors in determining whether advance care planning took place. The generalizability of our results is also a concern because the local population is largely white and highly educated, although our experience tells us that many of our program patients have limited means and thus may more closely resemble the general US population.44 The strength of our study is that it uses real, practice-based data that can be directly translated to practice.