Care Transitions Program for High-Risk Frail Older Adults is Most Beneficial for Patients with Cognitive Impairment





BACKGROUND: Although posthospitalization care transitions programs (CTP) are highly diverse, their overall program thoroughness is most predictive of their success.
OBJECTIVE: To identify components of a successful homebased CTP and patient characteristics that are most predictive of reduced 30-day readmissions.
DESIGN: Retrospective cohort.
PATIENTS: A total of 315 community-dwelling, hospitalized, older adults (≥60 years) at high risk for readmission (Elder Risk Assessment score ≥16), discharged home over the period of January 1, 2011 to June 30, 2013.
SETTING: Midwest primary care practice in an integrated health system.
INTERVENTION: Enrollment in a CTP during acute hospitalization.
MEASUREMENTS: The primary outcome was all-cause readmission within 30 days of the first CTP evaluation. Logistic regression was used to examine independent variables, including patient demographics, comorbidities, number of medications, completion, and timing of program fidelity measures, and prior utilization of healthcare.
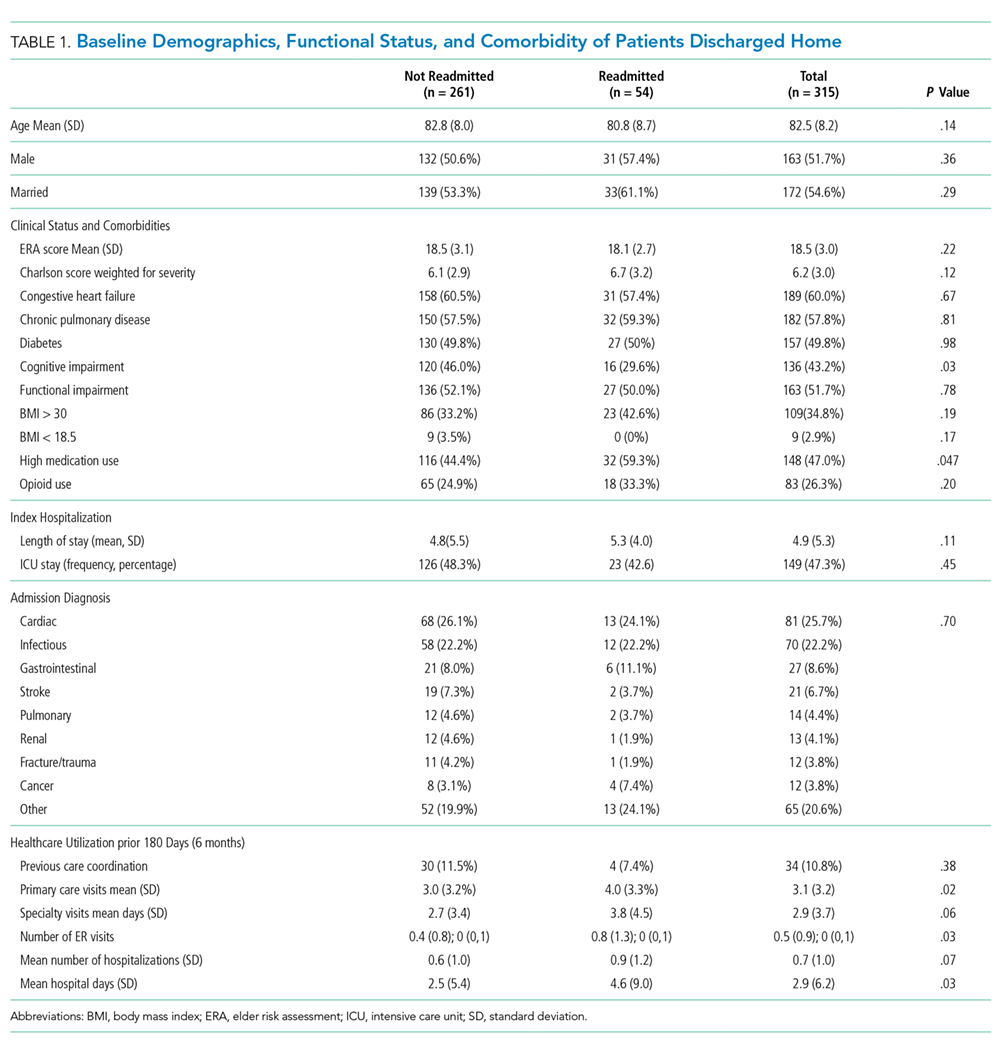
RESULTS: The overall 30-day readmission rate was 17.1%. The intensity of follow-up varied among patients, with 17.1% and 50.8% of the patients requiring one and ≥3 home visits, respectively, within 30 days. More than half (54.6%) required visits beyond 30 days. Compared with patients who were not readmitted, readmitted patients were less likely to exhibit cognitive impairment (29.6% vs 46.0%; P = .03) and were more likely to have high medication use (59.3% vs 44.4%; P = .047), more emergency department (ED; 0.8 vs 0.4; P = .03) and primary care visits (4.0 vs 3.0; P = .018), and longer cumulative time in the hospital (4.6 vs 2.5 days; P = .03) within 180 days of the index hospitalization. Multivariable analysis indicated that only cognitive impairment and previous ED visits were important predictors of readmission.
CONCLUSIONS: No single CTP component reliably predicted reduced readmission risk. Patients with cognitive impairment and polypharmacy derived the most benefit from the program.
© 2019 Society of Hospital Medicine
Independent Variables
Patient characteristics and clinical variables were retrieved from the EHR and included patient age, sex, and marital status. Comorbidities, ERA score,19 and Charlson comorbidity index (CCI)20 within two years of program enrollment were determined by using ICD-9 billing codes. The frequencies of primary care and specialty visits within six months of the index hospitalization were also ascertained using the EHR. Mobility limitations and cognitive impairment were categorized as binary variables (yes/no) and were assessed at the first home visit by the NP. The presence of mobility limitations was defined as a Barthel’s score of <7521,22 or Timed up and Go time of >20 seconds.23 Cognitive impairment was established as Kokmen below the normal cutoff for patient’s age group,24 Mini-Cog ≤2,25or AD8 ≥2.26 If these measures were not specifically documented during the first visit, clinical notes were queried for the description of pertinent cognitive and/or mobility limitations. Dementia diagnosis billing codes (ICD9 Code 290.*) were also included. High medication use was defined as >14 given the reported average medication number ranges from 8-13 in this population.27
As previously published, fidelity measures were abstracted from clinical notes by a trained nurse abstractor within 30 days of program enrollment and prior to a readmission.7 The five program fidelity measures included medication reconciliation, home service evaluation, advanced directives discussion, action plan for acute and chronic disease, safety plan, and discussion of community resources. The presence of advanced care planning was determined on the basis of visit medical notes and/or change of code status within the EHR, the identification or scanning of written advanced directives or “provider order for life-sustaining treatment,” and documentation of the discussion of resuscitation status. It was abstracted in duplicate by a nurse abstractor with physician adjudication for disagreement. Moreover, whether the initial visit met the goal of being within five days of discharge was determined by using billing data.
Analysis
The contribution of each independent variable to 30-day readmission was first directly assessed by using a univariate logistic regression model. Five patients died within 30 days without being admitted. These deaths, however, were not censored given that home death (as opposed to hospital death) was considered a positive outcome of the CTP. Multivariable modeling was performed through log rank test with backwards elimination and included all independent variables with P < .05. Variables with P values between .05 and >.1 were tested for interaction with age and sex. Age was categorized as <80 or ≥80 years. The length of hospital stay was categorized as <3 days (not qualifying for a Medicare skilled nursing facility), 3-13 days, or ≥14 days.
This study had 30% power to detect a reduction of 5% in the rates of hospital admissions; 5% is the median absolute risk reduction reported by previous randomized studies on care transitions programs previously reported.10 All analyses were performed using SAS 6.01 (SAS Inc., Cary, North Carolina).
RESULTS
Study Population
The study cohort included 315 patients who met the inclusion criteria (Fig 1). The demographic and clinical characteristics of the participants were ascertained at the time of CTP enrollment and are shown in Table 1. Patients were, on average, 82.5 (SD, 8.2) years old and had multiple comorbidities with a mean CCI score of 6.2 and ERA score of 18.5. Almost half of the patients (43.2%) exhibited cognitive impairment and more than half (51.7%) had mobility limitations. Among the patients, 42.9% had been hospitalized at least once in the 180 days prior to their CTP-qualifying hospitalization and 14.2% had ≥2 hospitalizations prior to their CTP-qualifying hospitalization. Similarly, 32.4% had at least one emergency department (ED) visit, and 3.5% had ≥3 ED visits. The majority of patients had frequent outpatient visits, with 30.8% having ≥4 office visits in primary care and 32.4% having ≥4 specialty office visits in the preceding six months.