Care Transitions Program for High-Risk Frail Older Adults is Most Beneficial for Patients with Cognitive Impairment





BACKGROUND: Although posthospitalization care transitions programs (CTP) are highly diverse, their overall program thoroughness is most predictive of their success.
OBJECTIVE: To identify components of a successful homebased CTP and patient characteristics that are most predictive of reduced 30-day readmissions.
DESIGN: Retrospective cohort.
PATIENTS: A total of 315 community-dwelling, hospitalized, older adults (≥60 years) at high risk for readmission (Elder Risk Assessment score ≥16), discharged home over the period of January 1, 2011 to June 30, 2013.
SETTING: Midwest primary care practice in an integrated health system.
INTERVENTION: Enrollment in a CTP during acute hospitalization.
MEASUREMENTS: The primary outcome was all-cause readmission within 30 days of the first CTP evaluation. Logistic regression was used to examine independent variables, including patient demographics, comorbidities, number of medications, completion, and timing of program fidelity measures, and prior utilization of healthcare.
RESULTS: The overall 30-day readmission rate was 17.1%. The intensity of follow-up varied among patients, with 17.1% and 50.8% of the patients requiring one and ≥3 home visits, respectively, within 30 days. More than half (54.6%) required visits beyond 30 days. Compared with patients who were not readmitted, readmitted patients were less likely to exhibit cognitive impairment (29.6% vs 46.0%; P = .03) and were more likely to have high medication use (59.3% vs 44.4%; P = .047), more emergency department (ED; 0.8 vs 0.4; P = .03) and primary care visits (4.0 vs 3.0; P = .018), and longer cumulative time in the hospital (4.6 vs 2.5 days; P = .03) within 180 days of the index hospitalization. Multivariable analysis indicated that only cognitive impairment and previous ED visits were important predictors of readmission.
CONCLUSIONS: No single CTP component reliably predicted reduced readmission risk. Patients with cognitive impairment and polypharmacy derived the most benefit from the program.
© 2019 Society of Hospital Medicine
Readmissions, Mortality, ED, and Outpatient Visits
Of the 315 patients, 54 (17.1%) had a readmission within 30 days and seven (2%) had >1 readmission. Among the patients, 126 (40.0%) were readmitted at least once within 180 days with 55 (17.5%) having more than one readmission. A total of 41 patients (13.1%) died during the six-month follow-up period. The need for both office and ED visits was reduced compared to the 180 days prior to admission with the biggest difference in ED visits: 72 (22.9%) of patients needed visits within 180 days of enrollment, as opposed to 102 (32.4%) before enrollment.
Impact of Patient Clinical Variables on Readmission Risk
Readmitted patients were less likely to exhibit cognitive impairment (29.6% vs 46.0%; P = .03) and were more likely to have high medication use (59.3% vs 44.4%; P = .047) than patients without readmission (Table 1). Readmitted patients had a higher frequency of visits to primary care (4.0 vs 3.0; P =.02) in the six months prior to admission and more hospital days in the prior year (4.6 vs 2.5; P = .04) than those without readmission.
Multivariable analysis, which included the cognitive status of the patient; the high use of medication; and the number of ED visits, primary care visits, and hospital days in the previous six months, provided a C statistic of 0.665. After backwards elimination, only the cognitive status of the patient and number of ED visits remained predictive of readmission risk.
Impact of Program Interventions on Readmission Risk
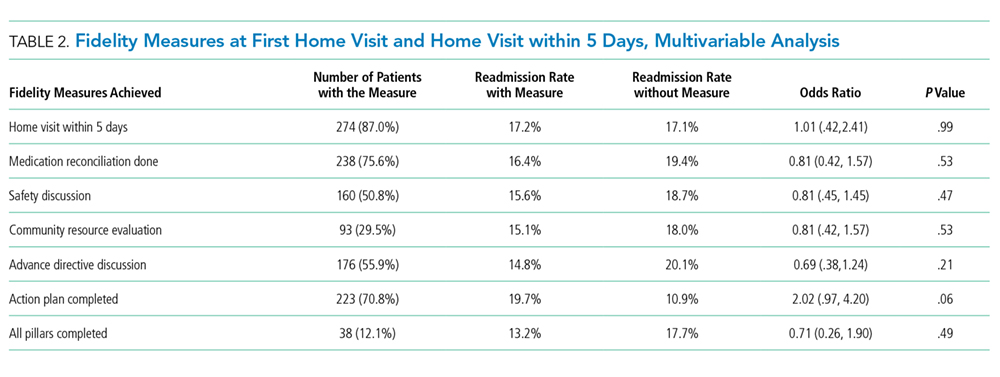
The completion of the CTP fidelity measures drastically varied with completion rates between 29.5% (community resource evaluation) and 87.0% (home visit within five days of hospital discharge; Table 2). Only 12.1% of patients received all components of the CTP at the first home visit. Readmission rates among patients who received all program components (13.2%) were lower than those among patients who did not receive all program components. This difference, however, failed to reach statistical significance. No single program component significantly reduced readmission risk. The completion rate of program fidelity measures increased with time (Figure 2). The present findings did not change even after performing sensitivity analysis that excluded the first program year. The overall agreement between chart abstractors on determining whether advance care planning occurred was 69.5% but the Cohens Kappa was only 18.4. This result was largely ascribed to the following: One abstractor counted the presence of a shorthand template used to document the delivery of an advance care planning document as discussion, whereas the other abstractor required further documentation or corroborating evidence (ie, change of code status). The majority of patients required multiple home visits to address ongoing medical needs (mean 2.7; SD = 1.3) over the first 30 days. Among these patients, only 17.1% received one visit, and 54.6% of patients received ≥3 visits. Eleven (3.5%) patients transitioned to a palliative homebound program that we began offering toward the end of this study to meet patient needs.28