Care Transitions Program for High-Risk Frail Older Adults is Most Beneficial for Patients with Cognitive Impairment





BACKGROUND: Although posthospitalization care transitions programs (CTP) are highly diverse, their overall program thoroughness is most predictive of their success.
OBJECTIVE: To identify components of a successful homebased CTP and patient characteristics that are most predictive of reduced 30-day readmissions.
DESIGN: Retrospective cohort.
PATIENTS: A total of 315 community-dwelling, hospitalized, older adults (≥60 years) at high risk for readmission (Elder Risk Assessment score ≥16), discharged home over the period of January 1, 2011 to June 30, 2013.
SETTING: Midwest primary care practice in an integrated health system.
INTERVENTION: Enrollment in a CTP during acute hospitalization.
MEASUREMENTS: The primary outcome was all-cause readmission within 30 days of the first CTP evaluation. Logistic regression was used to examine independent variables, including patient demographics, comorbidities, number of medications, completion, and timing of program fidelity measures, and prior utilization of healthcare.
RESULTS: The overall 30-day readmission rate was 17.1%. The intensity of follow-up varied among patients, with 17.1% and 50.8% of the patients requiring one and ≥3 home visits, respectively, within 30 days. More than half (54.6%) required visits beyond 30 days. Compared with patients who were not readmitted, readmitted patients were less likely to exhibit cognitive impairment (29.6% vs 46.0%; P = .03) and were more likely to have high medication use (59.3% vs 44.4%; P = .047), more emergency department (ED; 0.8 vs 0.4; P = .03) and primary care visits (4.0 vs 3.0; P = .018), and longer cumulative time in the hospital (4.6 vs 2.5 days; P = .03) within 180 days of the index hospitalization. Multivariable analysis indicated that only cognitive impairment and previous ED visits were important predictors of readmission.
CONCLUSIONS: No single CTP component reliably predicted reduced readmission risk. Patients with cognitive impairment and polypharmacy derived the most benefit from the program.
© 2019 Society of Hospital Medicine
METHODS
Study Design and Setting
This study is a retrospective cohort study of patients who were enrolled in the care transitions program of Mayo Clinic Rochester during the period January 1, 2010 to June 30, 2013. Patient demographic and clinical data were obtained from electronic health records (EHR), and information regarding CTP processes and interventions was obtained from a prospectively maintained program database. The study complied with the principles of the Declaration of Helsinki and was approved by the Mayo Clinic Institutional Review Board.
Objectives
The study aimed to describe the performance and utilization of a multidisciplinary care transitions program that has been successful in reducing readmissions for high-risk patients. The study also sought to identify patient and/or program factors associated with failure to prevent readmission within 30 days of program enrollment.
Population
Patients who were enrolled in the CTP following hospital discharge and seen for a posthospital in-home visit prior to hospital readmission (for those readmitted) were included. Patients discharged to a skilled nursing facility were excluded. Patients were eligible for CTP enrollment if they were hospitalized for any cause, community dwelling (including assisted living) prior to hospitalization, and ≥60 years old with an Elder Risk Assessment (ERA) score ≥16.7 The ERA incorporates information regarding previous hospital days, age, and comorbid health burden and has been shown to predict 30-day readmissions, mortality, and critical illness (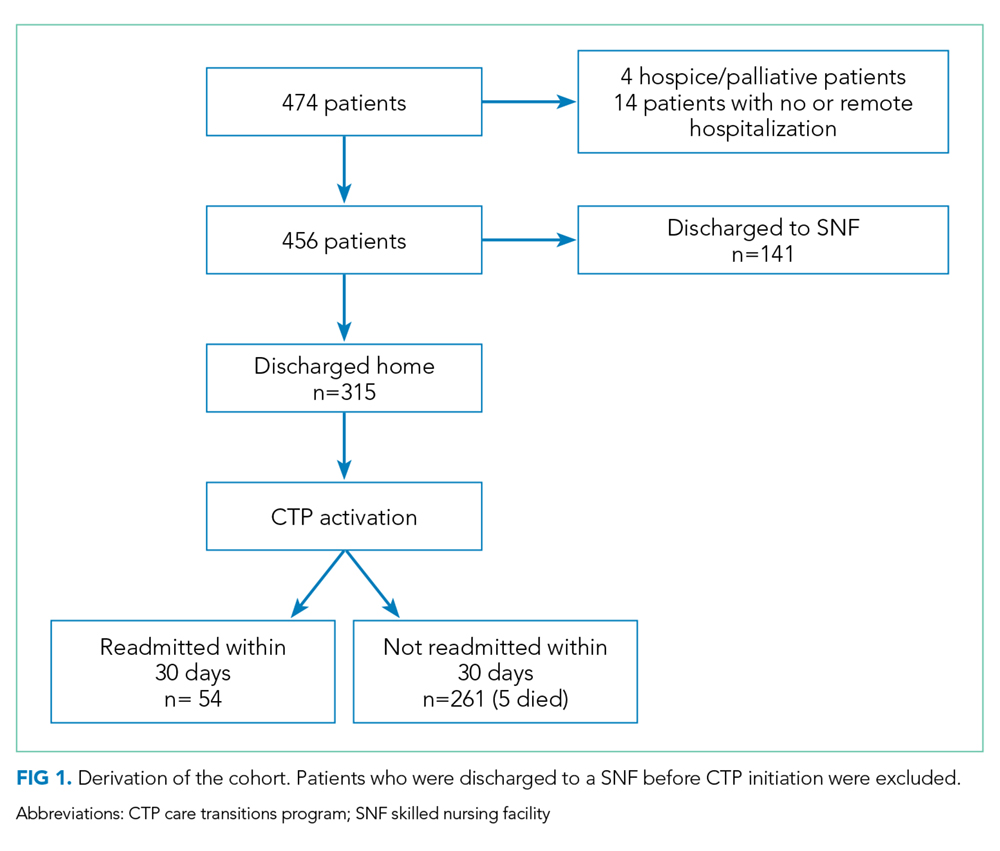
Intervention
Detailed descriptions of the CTP have been previously published.7,17 Patients meeting enrollment criteria are enrolled into the CTP by a RN prior to or immediately after hospital discharge. The patient is then seen at home within one to five business days of discharge and again the following week by a NP who performs medication reconciliation; chronic illness management; and acute illness, mobility, safety, and cognition assessments. The NP also provides patient education on self-care and advance care planning. Patient and caregiver support and liaisons with community resources are provided. Home visits by an NP or MD are continued as needed for at least one month. A RN case manager performs weekly phone calls to assess changes in the patient’s clinical status and is available for phone triage of acute health issues. An interdisciplinary team composed of MDs, NPs, RNs, and pharmacists review patient management at weekly meetings. Although after-hours or weekend coverage for home visits are unavailable, an on-call primary care physician is available by phone at all times.
Primary Outcome
The primary outcome was all-cause hospital readmission within 30 days of the first CTP home visit, indicating successful program enrollment. Hospitalization was determined on the basis of billing codes from Mayo Clinic hospitals; this approach is 99% reliable in detecting readmissions for this population.18
Secondary Outcome Measures
Secondary outcome measures included six-month mortality and hospitalizations, as well as the number of hospital and ICU days and home, ED, primary care, and specialty office visits within 180 days after index hospitalizations as per the EHR. ED visits were counted only when they did not result in a hospital admission.