How best to manage treatment-resistant depression?





Should you augment the treatment regimen with lithium, thyroxin, or an atypical antipsychotic? This review will help you decide.
Olanzapine, combined with fluoxetine in a fixed-dose pill (Symbyax), is the other FDA-approved agent for treatment-resistant depression. Trivedi and colleagues showed a remission rate of 25.5% and side effects ranging from 10% to 40%.18
Risperidone (Risperdal) rivals the efficacy of the medications previously discussed, but starting doses and titration schedules vary widely, making it difficult to determine which treatment course would be most efficacious.19-21
Quetiapine (Seroquel) has produced mixed results in treatment-resistant patients. That may have been because some studies used lower daily doses—25 to 100 mg—vs 150 to 600 mg in other trials.22 Bauer found higher remission rates compared to placebo (36% vs 24%)23 while Garakani22 did not (49% for quetiapine vs. 63% for placebo when using an intention-to-treat analysis; a similar lack of efficacy was found if those who dropped out of the study were excluded; P<0.29). Garakani also found that dry mouth, sedation, and other side effects occurred in up to 76% of patients. (Of note: Most studies of atypical antipsychotics are industry funded.)
Mirtazapine has not been well studied
Unfortunately, there are very little data on mirtazapine (Remeron). When the drug was added to ongoing antidepressant therapy, a single double-blind, randomized controlled trial found significantly better response rates compared with placebo.24 One advantage of the drug was that it helped relieve the sexual side effects of ongoing selective serotonin reuptake inhibitor (SSRI) therapy.25
Folic acid and SAMe also haven’t been well studied
Up to 50% of Americans have low levels of central nervous system L-methylfolate, which is a key co-factor in monoamine neurotransmitter production. Although lower plasma folate has been linked to depression, folate supplementation as a primary treatment for major depression has not been well studied and its use in treatment-resistant depression is limited to 1 study by Alpert and colleagues.26 Using an open-label, nonplacebo-controlled design in which folinic acid—an activated form of folic acid—was compared with placebo, researchers found remission rates of 18%, which is not significantly higher than the placebo response seen in other studies.
Similarly, there’s limited research on S-adenosyl-L-methionine (SAMe). Using a similar open-label, nonplacebo-controlled design, Alpert found a 43% remission rate in patients with treatment-resistant depression. Side effects occurred in up to half of patients, prompting 6.6% of patients to leave the study.27
Omega-3 fatty acids: The news is mixed
Data are contradictory on the value of omega-3 fatty acid for major depression28,29 and the evidence to support its use in treatment-resistant depression is likewise limited and contradictory.30 Until the data are more consistent and robust, it’s unclear whether omega-3 fatty acid supplementation can benefit patients.
Exercise helps
Some studies suggest that exercise can have a dose-responsive effect on clinical depression.31 As a result, the Treatment with Exercise Augmentation for Depression (TREAD) trial is underway to examine whether it can augment drug therapy. Preliminary evidence suggests that 30 minutes of aerobic exercise most days of the week can be effective.32,33 (For more on exercise, see “Does exercise alleviate symptoms of depression?”)
Cognitive therapy helps patients, and there are no side effects
The STAR*D study showed equivalent efficacy in achieving remission (23% vs. 33%) when comparing augmentation with cognitive therapy and augmentation with medications, with a low rate of side effects seen for cognitive therapy.34 Notably, it took longer to achieve remission (55 vs 40 days) when cognitive therapy was added to antidepressants. (For more on the STAR*D trial, see “What we learned from the STAR*D trial”) It’s also worth mentioning that other researchers did not find similar results for augmentation when they compared cognitive behavioral and brief supportive psychotherapy with medication therapy only.35
The Sequenced Treatment Alternatives to Relieve Depression (STAR*D) study is noteworthy because of its size, duration, design, and impact on the treatment of depression.5 This was a multicenter study of 3671 patients with major unipolar depression. Remission was determined by 2 rating scales—HRSD17 and QIDS-SR16*—and side effects were measured at each visit. There was no placebo control, no consideration for atypical antipsychotic medications or other therapies, and randomization was limited.
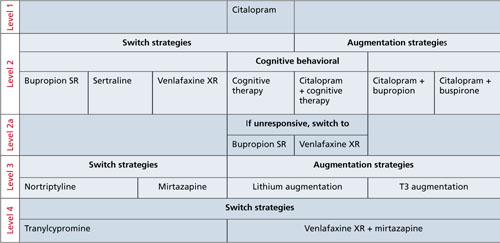
The FIGURE below shows how STAR*D was structured. In Level 1, patients were treated with citalopram (Celexa). If they didn’t go into remission, they were encouraged to proceed to Level 2, which involved 3 arms: switching agents, augmenting agents, or cognitive therapy. Patients chose which arm they wanted and were randomized to the specific medications used in that level. Switch agents included bupropion SR (Wellbutrin SR), sertraline (Zoloft), and venlafaxine XR (Effexor XR). Augmentation was with buspirone (BuSpar) and bupropion. Cognitive therapy was with or without continued citalopram with a second augmentation level of bupropion SR or venlafaxine XR. Level 3 also involved switch and augmentation arms using nortriptyline (Aventyl, Pamelor) or mirtazapine (Remeron) for switch agents and lithium or thyroxine for augmentation. Level 4 involved switching to tranylcypromine (Parnate) or venlafaxine XR plus mirtazapine.
Remission rates were 36.8% for those in Level 1, 30.6% in Level 2, 13.7% in Level 3, and 13% in Level 4. The cumulative remission rate was 67%. While remission rates for switch strategies in Levels 2 and 3 appeared to be lower for pharmacologic agents compared with augmentation strategies (27% vs 35% in Level 2 and 10.7% vs 20.5% in Level 3), the sample sizes were too small for the differences to be statistically significant, and the study was underpowered to establish the superiority of switch vs augmentation strategies.
Finally, it’s important to mention that patients of primary care physicians had similar remission rates, when compared with psychiatrists’ patients.42 Keep in mind, however, that the care provided in the STAR*D trial was structured and protocol-driven. After randomization into 1 medication group or another, dose adjustments were standardized at set intervals and based on inadequate response to validated depression severity assessment tools. Outcomes were patient-based and uniformly applied. This study structure may explain why remission rates were identical regardless of the specialty of the treating physician.
*The 17-item Hamilton Rating Scale of Depression and the 16-item Quick Inventory of Depressive Symptomatology–Self Report.
FIGURE
Structure of the Sequenced Treatment Alternatives to Relieve Depression (STAR*D)