Lesion on the hard palate





Our patient came in seeking relief from upper respiratory symptoms, but left with a referral to an oral surgeon.
Diagnosis: Perianal streptococcal dermatitis
The oral maxillofacial surgeon (TAC) concurred with the previous examination findings. He was concerned by the appearance of the lesion and the history of tobacco use and performed a biopsy of the lesion. The pathology report revealed that the patient had nicotine stomatitis with a concomitant candidiasis infection.
Nicotine stomatitis is a common mucosal keratosis caused by smoking tobacco. It is localized to the hard palate of the mouth, but can extend to the soft palate. The mucosa of the hard palate becomes white and thickened due to hyperkeratosis of the tissue.1 Thin red lines of normal mucosa can be seen throughout the lesion. Red dots or papules can appear in the center of the lesion, which represent irritated salivary glands with inflamed duct openings (FIGURE 2).2
Our patient’s lesion had an atypical presentation. Classically the lesions are whiter, but in this case, the patient’s lesion was more erythematous. The reason: A super-infection of candidiasis caused an atrophic form of the condition.
FIGURE 2
Classic presentation of nicotine stomatitis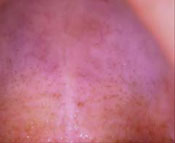
Differential Dx includes squamous cell carcinoma
The differential diagnosis in a case of nicotine stomatitis includes:
- irritation from dental appliances
- trauma from hot liquids
- squamous cell carcinoma
- atrophic candidiasis.
ill-fitting dentures can cause erythematous lesions along the hard palate and gingiva. The erythema from dentures is usually uniform in color without ulceration and follows the outline or shape of the oral appliance. In contrast, nicotine stomatitis will typically present on exposed areas of the palate and not follow any specific pattern. Most lesions caused by irritations or trauma resolve within 2 weeks of removal of the offending agent.