MANAGING CAP: An evidence-based algorithm





8 guidelines for site-of-care and treatment decisions
Diagnostic testing is of high yield for patients with severe CAP requiring ICU admission, allowing for early de-escalation of empirical treatment if results are negative.
FIGURE
Treatment of community-acquired pneumonia*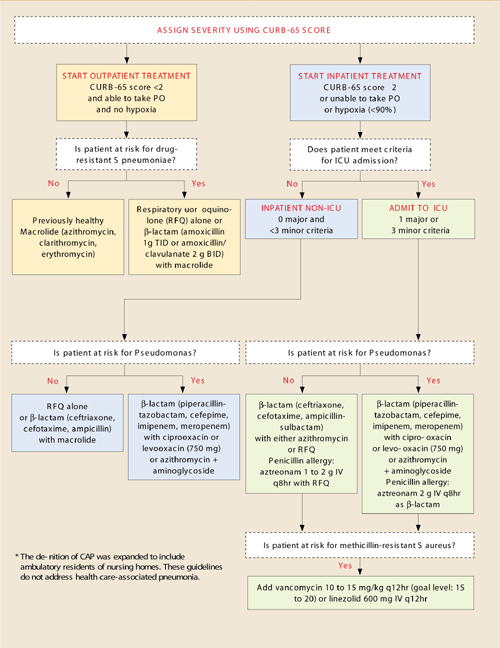
Adapted from: Mandell LA, Wunderink RG, Anzueto A, et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis 2007; 44(Suppl 2):S27–S72.
CURB-65 score for assessing severity of illness
Confusion
Uremia BUN >20
Respiration ≥30
BP <90/≤60 mm Hg
≥65 years of age
| TOTAL POINTS | MORTALITY RATE |
|---|---|
| 0 | 0.7% |
| 1 | 2.1% |
| 2 | 9.2% |
| 3 | 14.5% |
| 4 | 40.0% |
| 5 | 57.0% |
Criteria for ICU admission
Major
Invasive mechanical ventilation
Septic shock with need for vasopressors
Minor
- Respiration ≥30
- PaO2/FiO2 ≤250
- Multilobar infiltrates
- Disorientation
- BUN ≥20
- Hypotension requiring aggressive fluids
- Temperature <36°C
- Platelets <100,000
- WBC<4000
Risk factors
Drug-resistant S pneumoniae
- Any antibiotics within 3 months
- Comorbidities: Cardiac disease, diabetes mellitus, alcoholism, pulmonary disease, renal disease, liver disease, asplenia, malignancy, immunosuppressed.
- age >65 years
Pseudomonal infection
- Structural lung disease (bronchiectasis)
- Severe COPD with frequent admissions, recent antibiotic and steroid use
Methicillin-resistant S aureus
Pulmonary abscess
End-stage renal disease
IV drug abuse
Recent influenza
Recent fluroquinolone use
Duration of antibiotic treatment
- At least 5 days
- After 5 days, antibiotics may be discontinued when patient is afebrile 72 hours and has no more than 1 criteria for instability: temperature ≥37.8°C, heart rate ≥100, respiration ≥24, systolic BP ≤90 mm Hg, O2 saturation ≤90%, inability to maintain oral intake, altered mental status
- 15 days for CAP due to Pseudomonas
Criteria for discharge
Temperature ≤37.8°C, heart rate ≤100, respiration ≤24, systolic BP ≥ 90 mm Hg,O2 saturation ≥90%, ability to maintain oral intake, normal mental status
Pathogen-directed therapy
6. Identify the pathogen
New guidelines recommend that, once the pathogen is identified by reliable microbiological methods, therapy should be directed towards that specific pathogen to prevent increased resistance in the community (moderate recommendation, level III evidence).
Influenza. Treatment within 48 hours of symptom onset with oseltamivir or zanamivir is recommended for influenza A (strong recommendation, level I evidence).
While these antimicrobials should not be used in uncomplicated influenza with symptoms for >48 hours (level I evidence), they may be used in hospitalized patients or influenza pneumonia to reduce viral shedding (moderate recommendation, level III evidence).
LEVEL I HIGH
Well-conducted, randomized controlled trials
LEVEL II MODERATE
Well-designed, controlled trials without randomization (including cohort, patient series, and case-controlled studies); large case series in which systematic analysis of disease patterns and/or microbial etiology was conducted; and reports of data on new therapies that were not collected in a randomized fashion.
LEVEL III LOW
Case studies and expert opinion. In some instances, therapy recommendations may come from antibiotic susceptibility data without clinical observations.
Adapted from: Mandell et al.1
Time to first dose
7. Start treatment in the ED
Rather than designating a time window for starting treatment, the IDSA/ATS committee recommended that patients receive the first antibiotic dose in the Emergency Department (moderate recommendation, level III evidence).
This newly added statement contrasts with some current quality measures that grade hospitals according to whether antibiotics are started within a specific time frame.
Duration of antibiotics
8. Base duration on specific criteria
Reflecting evidence that shorter courses appear to be as effective as longer courses, the newer guidelines recommend discontinuation when the patient meets specific clinical criteria. Before discontinuing antibiotics, all patients with CAP should:
- Be treated for at least 5 days (level I evidence),
- Be afebrile for 48 to 72 hours, and
- Have no more than 1 of these criteria for clinical instability (moderate recommendation, level II evidence): temperature ≥37.8°C; heart rate ≥100 beats/min; respiratory rate ≥24 breaths/min; systolic blood pressure ≤90 mm Hg; arterial oxygen saturation ≤90% or pO2 ≤60 mm Hg on room air; inability to maintain oral intake; altered mental status.
Switching from IV to oral
The guidelines, similar to the prior guidelines, recommend switching to oral therapy for hemodynamically stable patients who are clinically improving, able to ingest medications, and have a normally functioning gastrointestinal tract (strong recommendation, level II evidence).
Hospital discharge
The guidelines recommend that patients be discharged as soon as they are clinically stable and have a safe environment for continued care. Patients receiving oral therapy do not require inpatient observation (moderate recommendation, level II evidence). This is unchanged from prior recommendations.