Stress tests: How to make a calculated choice





Spare your patients unnecessary stress testing by determining their pretest probability for CAD.
Equivocal. Reports that come back as equivocal will have ECG changes nondiagnostic of ischemia such as alterations in P- or T-wave morphology and nondiagnostic changes in AV conduction, particularly if changes revert to baseline during the rest period. Unifocal PACs or PVCs (<5/min) are not specific indicators for CAD and the development of bundle branch blocks are nondiagnostic findings. Equivocal results need additional testing such as myocardial perfusion imaging or angiography to document ischemia if the pretest probability is high.
Incomplete or failure. If your patient’s test involves equipment failure or if he (or the operator) was unable to complete the test, you should get a report to that effect. Depending on the nature of the failure, you may need to repeat the test, consider PSMI, or make a cardiology referral.
Duke Treadmill Score
A helpful calculation following treadmill testing
If your patient had a positive or negative exercise treadmill test, consider calculating his Duke Treadmill Score (DTS), which is predictive of 5-year survival and significant severe CAD for patients who are younger than 75 years.4,14
DTS helps you to exclude low-risk patients from further invasive testing and ensure high-risk patients receive further evaluation and appropriate treatment. DTS appears to be more useful in women with an intermediate pretest score but not with a low pretest score.15
The DTS score typically ranges from –25 to +15.5 Patients at low risk will have a score of > +5), moderate risk will have scores ranging from –10 to +4, and those at high risk will have a score of ≤–11.4
A modified DTS is used for patients older than 65 years who may have a limited exercise capacity, controlled asymptomatic congestive heart failure, or be on digoxin, which may affect their ability to perform a maximal exercise treadmill test.5 The values for the Elderly Alternative Treadmill Score are as follows: low risk (< –2); moderate risk (–2 to 2); and high risk (>2). (See “The calculations behind the scores.”)
Bottom line
DTS scores, Elderly Alternative Treadmill Scores, and pre–stress test CAD probability scores are all extremely useful. Integrating them into your practice can ensure that patients get the prompt care they may need, while sparing them unnecessary tests along the way.
FIGURE
Template for dictating noninvasive cardiac tests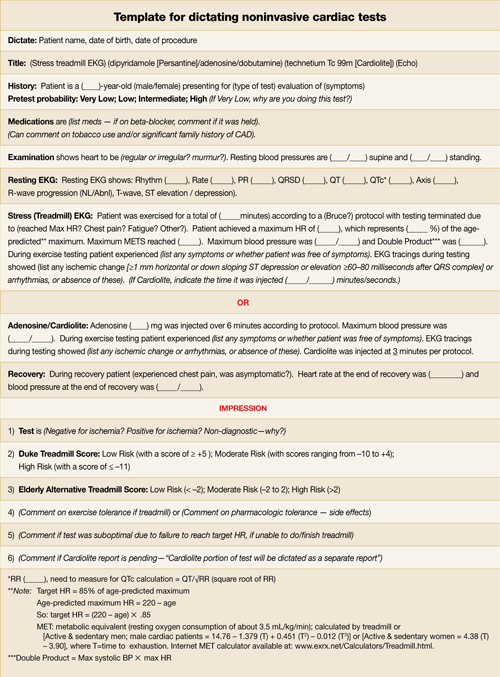
Correspondence
Dennis P. Breen, MD, Eau Claire Family Medicine Clinic, 617 Clairemont Avenue, Eau Claire, WI 54701. dennis.breen@fammed.wisc.edu