Open-angle glaucoma: Tips for earlier detection and treatment selection





Beta-adrenergic antagonists can lower IOP by up to 31% 25 and are often used as first-line treatment (SOR: A).21 However, nonselective beta-blockers (timolol, carteolol, levobunolol, metipranolol) are associated with a number of adverse effects including bronchospasm,33 bradycardia, and hypotension. 34
Betaxolol is a selective beta-blocker with less tendency to cause pulmonary side effects,34 but it may still do so in patients with severe pulmonary disease.35 Selective beta-blockers lower IOP to a lesser degree than nonselective drugs36 and can cause the same cardiac effects of bradycardia and hypotension.38
Prostaglandin analogs (latanoprost, travoprost, unoprostone) increase drainage of the aqueous humor. Prostaglandins are clinically and statistically superior to beta-blockers, having lowered IOP by up to 40% in randomized controlled trials.37 Side effects include increased eyelash growth and iris pigmentation,26 and muscle and joint pain.38
Alpha-adrenergic drugs (apraclonidine, brimonidine) lower aqueous humor production. Apraclonidine administered topically does not cross the blood-brain barrier, effectively lowering IOP without causing cardiovascular side effects.28 The most common side effects are dry nose, dry mouth,28 and follicular conjunctivitis.29 Unlike apraclonidine, brimonidine crosses the blood-brain barrier and can cause mild hypotension.30 One randomized controlled trial found no statistical difference in efficacy between brimonidine and apraclonidine, both lowering IOP by up to 23%.39
Carbonic anhydrase inhibitors block water flow into the eye, preventing aqueous humor formation. Until recently, carbonic anhydrase inhibitors such as acetazolamide were administered only orally and adverse effects were therefore common.27 Topical carbonic anhydrase inhibitors (brinzolamide, dorzolamide), recently introduced, lower IOP by up to 26% and with few side effects.31
Cholinergic agonists (pilocarpine, carbachol) increase aqueous outflow from the eye by stimulating contraction of the ciliary body, which opens the trabecular meshwork to allow further drainage.40 Because of its ocular side effects including small, fixed pupils, induced myopia, and cataracts, pilocarpine is reserved for second-or third-line therapy (SOR: A). 9,27,32
Medicinal marijuana used to lower IOP in glaucoma patients is controversial. The primary active ingredient in marijuana, tetrahydrocannabinol (THC), lowers IOP when inhaled. However, it lowers IOP for only 3 hours, and glaucoma management requires a constant reduction in IOP. Due to its intense side effects of altered mental status, tachycardia, and systemic hypotension, medicinal marijuana is not desirable for the treatment of glaucoma.41
Benefit in combining regimens. Using different classes of drugs produces an additive effect in lowering IOP, so the ophthalmologist may use up to 3 drugs simultaneously. When therapy is begun, a topical drug is often applied to only 1 eye, letting the opposite eye serve as a control. If IOP is not lowered in the treated eye when compared with the control eye, the drug is discontinued (SOR: A).27
Dealing with noncompliance. More than one third of patients exhibit poor compliance with therapy,9 and strict adherence to the regimen is necessary to lower IOP. Instruct patients in proper techniques for taking and using medications, and record dosage and frequency at each physician visit.
Advise patients that glaucoma can progress, but that blindness is not inevitable. Stress the importance of adhering to the prescribed treatment regimen (SOR: C). 13 If poor compliance remains an issue, let the patient know that therapeutic alternatives may be possible (SOR: C). 2
Argon laser trabeculoplasty
Argon laser trabeculoplasty (ALT) is an outpatient procedure. Laser energy is directed at the trabecular meshwork to facilitate aqueous humor outflow. In a large clinical trial with long-term follow-up, initial ALT therapy was found to be at least as effective as initial pharmacological treatment.42
Medical treatment is often continued after ALT.43 In the Early Manifest Glaucoma Trial,25 glaucoma patients randomized to receive ALT therapy plus a topical beta-blocker (betaxolol) had a 30% reduction in IOP. Compared with the control group, patients treated with ALT and beta-blocker exhibited half the risk of visual field deterioration, with a number needed to treat of 2.24 to prevent field loss in a patient with a baseline IOP of 24 mm Hg.
Surgery
Although surgical treatment is generally considered a final alternative in management, it may be an appropriate first-line therapy for patients with cardiovascular or pulmonary conditions contraindicating use of medical therapy. 13
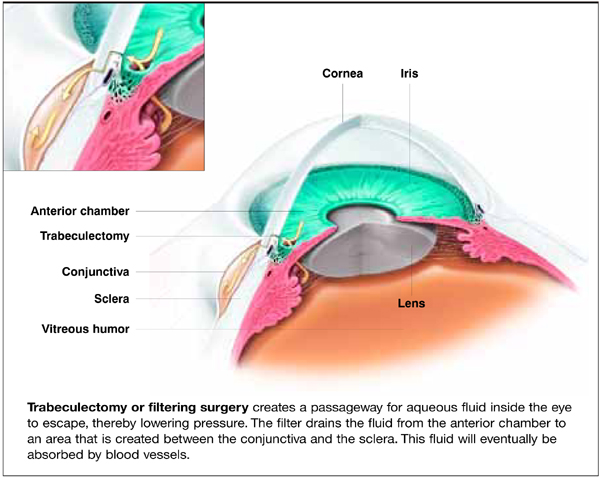
Filtering surgery (trabeculectomy) (Figure) is an outpatient procedure wherein IOP is lowered by creating a fistula in the globe of the eye to drain aqueous humor into the sub-conjunctival space.21 In a randomized controlled trial, trabeculectomy used alone or with medical therapy in a previously unoperated eye successfully lowered IOP by a rate of 85% to 95% at 2 years.44 At 5 years, the success rate in Caucasians is 90%; in African Americans, 80%.44 However, a recent meta-analysis suggests that glaucoma surgery is associated with accelerated progression of cataract.45 The Collaborative Initial Glaucoma Treatment Study (CIGTS) found 3 times the incidence of cataract surgery among subjects randomized to initial filtration surgery as opposed to medical management (P=.0001).46
FIGURE
Filtering surgery for glaucoma