
Evaluation of suspected left ventricular systolic dysfunction





Echocardiography. The most important step in the evaluation of the heart failure patient is the assessment of left ventricular systolic function. Both echocardiography and radionuclide ventriculography have been advocated.8-14 However, echocardiography is preferred as it is widely available, simple, noninvasive, safe, usually less expensive, and provides more information about valve function and left ventricular hypertrophy. Table 2 demonstrates the high sensitivity and specificity of echocardiography.35 In view of this, it is recommended as a standard adjunct to the clinical diagnosis of patients with dyspnea on exertion and suspected heart failure. Between 8% and 18% of patients will have inadequate echocardiograms, in which case radionuclide ventriculography is advocated.8
Neurohormonal markers. In recent years there has been increasing interest in the potential role of neurohormonal markers, such as B-type natriuretic peptide (BNP), atrial natriuretic peptide (ANP), N-terminal pro-ANP (N-ANP), and N-terminal pro-BNP (N-BNP) as indices of LVSD.36-42 Most of the data relating to these markers are relatively recent; therefore their use is not addressed in any detail in any of the aforementioned guidelines.
Some studies41,42 suggest that BNP and N-BNP are useful for diagnosing LVSD even when the positive predictive values are low, because of their high negative predictive values. One of the most recent studies44 examined the utility of BNP in an urgent care setting and suggested that BNP was an extremely reliable indicator of LVSD. In this population of patients with acute dyspnea where 39% had a final diagnosis of heart failure, 90% with a positive BNP had heart failure and 98% of those with a negative BNP did not. Although there appears to be a growing body of evidence supporting the role of these neurohormonal markers in the evaluation of the patient with LVSD, Table 2 illustrates that there have also been conflicting findings. This is partly because of differences in study design, study populations, cut-off points for ANP and BNP, and the definition of LVSD. Most studies agree that assessment of BNP, in particular, may be a cost-effective method for initial screening for LVSD, but should still be followed by an echocardiogram to confirm the diagnosis.
Management follows diagnosis. Making the correct diagnosis is the crucial first step in the management of chronic heart failure. Figure 1 summarizes the steps currently recommended for the evaluation of the patient with LVSD. A confirmation of a diagnosis of LVSD, however, is not the end of the story. Management will then need to include initiation of appropriate therapies and consideration of treatable and reversible etiologies, a subject to be addressed in the June 2002 issue of this journal.
TABLE 2
Key investigations used for the diagnosis of left ventricular systolic dysfunction
| Test | N | Setting* | Study quality † | Sensitivity (%) | Specificity(%) | LR+ | LR- | PV+ (%) | PV- (%) |
|---|---|---|---|---|---|---|---|---|---|
| Electrocardiogram | |||||||||
| Davie, 199729 | 534 | R | 1c | 94 | 61 | 2.43 | 0.10 | 35 | 98 |
| Lindsay, 200043 | 416 | R | 1c | 90 | 65 | 2.59 | 2.76 | 43 | 90 |
| Mosterd, 199732 | 1980 | R | 1c | 54 | 79 | 2.55 | 0.58 | 7 | 98 |
| Electrocardiogram (patient older than 70 years) | |||||||||
| Mosterd, 199732 | 1980 | R | 1c | 67 | 64 | 1.88 | 0.52 | 7 | 98 |
| Talreja, 200030 | 330 | H | 1c | 65 | 98 | 38.2 | 0.36 | 98 | 64 |
| Chest x-ray | |||||||||
| Badgett, 199634 | 29 studies | 2a | 51 | 79 | 2.43 | 0.62 | 71 | 62 | |
| Rihal, 199524 | 554 | H | 2b | 20 | 89 | 1.82 | 0.90 | 34 | 79 |
| Echocardiogram | |||||||||
| Erbel, 198435 | 110 | H | 1c | 80 | 100 | 80.0 | 0.20 | 100 | 85 |
| N-terminal ANP > 4.4 ng/mL | |||||||||
| McClure, 199840 | 134 | M | 2b | — | — | 1.08 | 0.96 | 52 | 51 |
| N-terminal pro-BNP > 275 fmol/mL | |||||||||
| Talwar, 199942 | 249 | R | 2b | 94 | 55 | 2.09 | 011 | 58 | 93 |
| BNP > 75 pg/mL | |||||||||
| Maisel, 200137 | 200 | R | 1c | 86 | 98 | 43.0 | 0.14 | 98 | 89 |
| Dao, 200144 | 250 | U | 1b | 98 | 92 | 12.2 | 0.02 | 92 | 98 |
| BNP > 46 pg/mL | |||||||||
| McClure, 199840 | 134 | M | 2b | — | — | 2.25 | 0.83 | 69 | 55 |
| BNP > 17.9 pg/mL | |||||||||
| McDonagh, 199841 | 1653 | P | 2b | 76 | 87 | 5.85 | 0.28 | 16 | 97 |
| NOTE: Pretest probability = 50%. | |||||||||
| *P denotes cross-sectional primary care population; R, primary care patients referred for suspected heart failure; H, hospitalized patients undergoing angiography; U, urgent care center; M, long-term myocardial infarction survivors recalled by their family physician. | |||||||||
| † Level 1a is the most rigorous; level 5 is the least rigorous. | |||||||||
| ANP, atrial natriuretic peptide; BNP, B-type natriuretic peptide; LR+, positive likelihood ratio; LR-, negative likelihood ratio; PV+, positive predictive value; PV-, negative predictive value. | |||||||||
Figure
Steps in the assessment of the patient with suspected heart failure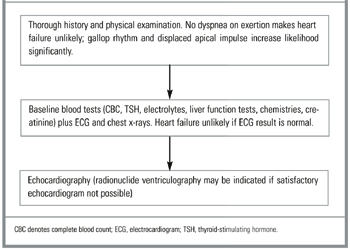
ACKNOWLEDGMENTS
We wish to thank Mr Chris Shiels at the Department of Primary Care, University of Liverpool, for his valuable advice regarding this manuscript.
