Do All Hospitals Need Cesarean Delivery Capability?





An Outcomes Study of Maternity Care in a Rural Hospital Without On-Site Cesarean Capability
The Zuni-Ramah Hospital limits intrapartum care to women designated as at low or moderate risk by criteria established by Zuni-Ramah family physicians and reviewed by GIMC OBGs. Criteria mandating transfer included prior cesarean, malpresentation, multiple gestation, intrauterine growth restriction, severe preeclampsia, placenta previa, significant vaginal bleeding, major fetal anomalies, anticipated preterm delivery (< 36 weeks), nonreassuring fetal heart tones (NRFHTs), and need for labor induction or augmentation with oxytocin. Women with gestational or type 2 diabetes who were well controlled could give birth at Zuni-Ramah unless they had end-organ damage or the fetus had known macrosomia. Physicians successfully completed the Advanced Life Support in Obstetrics (ALSO, ®American Academy of Family Physicians, 4th ed., 2000) course, attended weekly high-risk obstetric rounds, and performed quarterly reviews of obstetric complications. The family physicians performed vacuum-assisted deliveries, utilized amnioinfusion, and used continuous or intermittent fetal monitoring.
A review of the delivery and transfer records of the Zuni-Ramah Hospital and GIMC obstetric services revealed that there had been 1132 births of 1137 infants during the study period. The authors used a data collection form to review prenatal and newborn records from every birth. We reviewed intrapartum records for all births at the Zuni-Ramah and GIMC hospitals. We obtained discharge summaries from tertiary-care sites. We interviewed perinatal coordinators, public health nurses, and pediatric care providers to obtain information about patients who had received perinatal care outside of the IHS system.
The outcomes measured included perinatal mortality, neonatal morbidity, obstetric emergencies, intrapartum and antepartum transfers, and cesarean delivery rate. All obstetric emergencies originating at Zuni-Ramah Hospital were reviewed to determine whether the lack of surgical facilities had resulted in adverse outcomes. The physician’s notes were used to differentiate a NRFHT pattern requiring observation at a hospital with operative facilities from a truly worrisome pattern that required urgent intervention for fetal distress.
Births were defined as deliveries of infants at 20 weeks or more of estimated gestational age. We analyzed each birth in a multiple gestation individually. The population-based perinatal mortality rate was calculated from 20 weeks’ estimated gestational age to the 28th neonatal day. The Zuni-Ramah Hospital perinatal mortality rate was calculated by inclusion of all women delivered at Zuni-Ramah Hospital or transferred during labor. Approval for the study was obtained from the IHS Institutional Review Board and the Zuni Tribal Council.
Results
Study population
We identified 1137 births to 945 women between 1992 and 1996. Zuni and Navajo births were 66.9% and 30.8%, respectively; 30% of women were primiparous and 70%, multiparous. We found that 10.4% of births had occurred in women older than 35 years and 7.8% in women younger than 18 years. Regarding prenatal care, 3.9% of women had received none; 43.0% had established prenatal care in the first trimester; 40.4%, in the second trimester; and 12.8%, in the third trimester.
Delivery sites and maternal transfers
The majority of women (64.4%, n = 732) gave birth at the Zuni-Ramah Hospital (Figure) or at GIMC (29.6%, n = 337). A small number (2.2%, n = 25) gave birth at a private hospital with surgical facilities in Gallup. Albuquerque tertiary-care hospitals were the sites of 3.2% (n = 36) of deliveries. Primary indications for tertiary care were prematurity and fetal anomalies. Seven (0.6%) deliveries occurred at other sites, including home and ambulance.
The antepartum transfers (Table 1) were required primarily for pregnancy complications requiring labor induction. Preeclampsia, diabetes, nonreassuring antepartum testing, and post dates patients accounted for 56.8% of the 290 transfers. The 107 intrapartum transfers were made predominantly for labor induction or augmentation (64.5%, n = 69), a concerning fetal heart tracing (15.9%, n = 17), or fetal malpresentation diagnosed during labor (8.4%, n = 9).
FIGURE
PREGNANCIES AT ZUNI-RAMAH HOSPITAL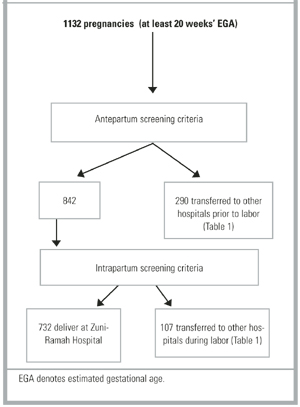
TABLE 1
ANTEPARTUM AND INTRAPARTUM TRANSFERS FROM ZUNI-RAMAH HOSPITAL
| Indication | Number of Transfers (%) |
|---|---|
| Antepartum Transfers* | |
| Preeclampsia | 83 (28.6) |
| Prior cesarean delivery | 55 (19.0) |
| Nonreassuring testing | 39 (13.4) |
| Preterm (includes PPROM) | 24 (8.3) |
| Diabetes | 22 (7.6) |
| Postdates | 21 (7.2) |
| Other | 18 (6.2) |
| Malpresentation | 16 (5.5) |
| Chronic HTN | 8 (2.8) |
| Macrosomia | 7 (2.4) |
| IUFD | 6 (2.1) |
| IUGR | 5 (1.7) |
| Anomalies | 4 (1.4) |
| Total | 290 (25.6% of population) |
| Intrapartum Transfers | |
| First-stage arrest of labor | 37 (34.6) |
| PROM without active labor | 32 (29.9) |
| Malpresentation | 9 (8.4) |
| Fetal distress | 5 (4.7) |
| Nonreassuring tracing | 12 (11.2) |
| Other | 12 (11.2) |
| Total | 107 (9.5% of population) |
| *Greater than 290 because of 18 patients with 2 reasons for antepartum transfer. | |
| HTN denotes hypertension; IUFD, intrauterine fetal demise; IUGR, intrauterine growth restriction; PROM, premature rupture of membranes; PPROM, preterm premature rupture of membranes. | |
Obstetric interventions
The total cesarean delivery rate (7.3%) was approximately one third the nationwide rate of 20.7% in 1996. The primary cesarean delivery rate (number of cesareans in women without prior cesarean divided by the number of women who have never had a cesarean) of 5.3% compares with a nationwide primary rate of 14.6%. The cesarean rate was 22.1% for antepartum transfers and 17.8% for intrapartum transfers. Operative vaginal delivery occurred in 5.4% of births, well below the nationwide rate of 9.4%. The induction rate of 13.8% is lower than the nationwide rate of 16.9%. The oxytocin augmentation rate of 7.7% is well below the nationwide rate of 16.9% in 1996.13 Parenteral narcotics were available at Zuni-Ramah; however, 81.4% of women elected to receive no labor analgesia. Epidural anesthesia was not available at Zuni-Ramah Hospital.