
Deep Endometriosis Compromising the Rectum - Diagnosis and Treatment





When the preoperative rectal ultrasound permits identification of the depth of the lesion, this information can be used to define the type of surgery that will be performed. In the case of unifocal lesions less than 3 cm in size (major diameter) and affecting the serous and external muscular layers of the rectum or sigmoid, resection of the nodule alone may be indicated. This procedure may be done manually or with the help of a circular stapler.
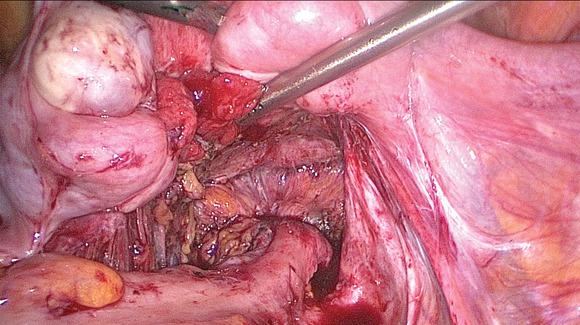
Our technique, approached laparoscopically, is as follows:
• The lesion on the rectosigmoid is delineated, and adhesions are lysed from contiguous organs such as adnexae, the uterus, or other loops of bowel. We prefer to use scissors or a hook.
• To resect the lesion manually (without the use of a disposable stapler), the endometriotic nodule is excised, taking care not to leave any residual disease behind. The defect is then repaired in a double-layer fashion. On the mucosal layer, 3-0 absorbable suture is used in a running and transverse manner to avoid bowel constriction. On the seromuscular layer, 3-0 permanent suture is used in a running manner to imbricate over the first layer.
• If a circular stapler is used, the following steps are followed: A stitch is placed in the lesion in order to invaginate it into the stapler. With the stapler inserted into the patient’s rectum, it is opened and the lesion is invaginated into the stapler. The stapler is then closed and fired.
• The anastomosis is tested in a same way as the closure is tested following more limited resection of a nodule (described above).
If, on the other hand, the lesion is deeper, affecting the deep muscle or the submucosal or mucosal layers, then segmental resection of the bowel is recommended. Complete surgical resection of endometrial foci has been shown to result in improved quality of life and decreased rates of recurrence (Fertil. Steril. 2004;82:878-84).
Segmental resection of the rectosigmoid can be performed laparoscopically (J. Minim. Invasive Gynecol. 2008;15:280-5). Our technique involves the following steps:
• Both ureters are identified before complete mobilization of the rectum and sigmoid 1 cm proximal and distal to the endometriotic lesion.
• The mesosigmoid is divided with an ultrasonic device.
• A linear stapler is utilized on the rectosigmoid distal to the lesion.
• After excision of all endometriotic implants, the right-lower trocar site is extended to 4 cm in order to remove the surgical specimen(s) and to prepare the proximal stump.
• An incision is made on the proximal stump in order to insert the anvil of the circular stapler.
• A purse-string suture holding the anvil in place is performed prior to replacement of the sigmoid into the abdominal cavity.
• The 4 cm fascial incision is closed in order to finish the procedure laparoscopically.
• The circular stapler is inserted through the anus in order to complete the end-to-end reanastomosis. The anastomosis is tested by gently injecting air and/or methylene blue through the rectum (with an Asepto, or large bulb syringe) while the surgeon occludes the proximal sigmoid with an atraumatic instrument. Absence of air bubbles and/or methylene blue while the anastomotic site is submerged in sterile water in the pelvis confirms a tight anastomosis.
• A large drain is left adjacent to the anastomosis prior to closure of trocar sites. The drain is generally removed 4 days postoperatively.

Deep endometriosis is associated with more severe pain and significantly greater rates of infertility, compared with superficial endometriosis. Because of the high risks of surgical intervention, preoperative diagnosis using imaging modalities can be helpful in planning surgical strategy. Improved outcomes are achieved with complete surgical resection, which can be performed through minimally invasive techniques.
Dr. Mauricio S. Abrão has been president of the Brazilian Society of Endometriosis and Minimally Invasive Endoscopy, and he has been a board member of the World Endometriosis Society since 1998. He currently is on the board of trustees of the AAGL and is the chairman of the society’s special interest group on endometriosis. Dr. Abrão is leading the AAGL initiative on producing a new classification on endometriosis. Dr. Abrão has nearly 100 papers published in peer-reviewed journals, the majority dealing with endometriosis. Dr. Abrão reported that he has no relevant financial disclosures.