Effectiveness and Safety of Droperidol Use in the VA Greater Los Angeles Healthcare System Emergency Department





Background: Droperidol, a butyrophenone antipsychotic, is used for postoperative nausea and vomiting and as a sedative, anxiolytic, and analgesic. Concerns about potential QTc (corrected QT interval) prolongation led the US Food and Drug Administration (FDA) to issue a boxed warning and halt manufacturing. However, recent studies have supported droperidol’s safety and it was reintroduced in 2019. Given the limited available options for managing acute agitation at the Veterans Affairs Greater Los Angeles Healthcare System (VAGLAHS), there has been interest in re-evaluating the risks associated with droperidol use for sedation, anxiolysis, analgesia, and as an antiemetic.
Methods: This retrospective chart review examined patients who received droperidol in the VAGLAHS emergency department (ED) from February 2021 to April 2023. The primary outcome was all-cause mortality after droperidol administration within 24 hours. Secondary outcomes included the efficacy of droperidol, incidence of QT prolongation, incidence of extrapyramidal symptoms (EPS) such as akathisia, dystonia, parkinsonism or tardive dyskinesia, and incidence of respiratory depression.
Results: Of 207 patients receiving droperidol, 38 (18.4%) were adults aged ≥ 65 years. Droperidol was used for acute agitation in 183 patients (88.4%) and as an antiemetic in 24 (11.6%) patients. No deaths were observed following droperidol administration in a 24-hour period. The need for rescue medication occurred in 15 patients (7.3%). EPS such as tardive dyskinesia and dystonia occurred in 2 (1.0%) patients. No arrhythmias or respiratory depression were observed within 24 hours of administration. No clinically relevant QTc prolongation was observed.
Conclusions: No fatalities were seen among patients who received droperidol in the VAGLAHS ED. Despite the boxed warning issued by the FDA, these findings suggest droperidol is safe and effective in managing agitation and as an antiemetic.
Droperidol is a butyrophenone antipsychotic approved by the US Food and Drug Administration (FDA) for use in postoperative nausea and vomiting (PONV). Off-label, it has also been utilized for its sedative, anxiolytic, and analgesic properties.1 While its exact mechanism of action remains elusive, it is believed that binding to postsynaptic γ-aminobutyric acid receptors induces anxiolysis and sedation, while dopaminergic activity in the chemoreceptor trigger zone contributes to its antiemetic effects.2 Since the introduction of droperidol in 1967, it has been widely used by emergency physicians, psychiatrists, and anesthesiologists globally.1
Despite its therapeutic efficacy, use of droperidol has been tempered by concerns regarding its cardiovascular safety profile, specifically its potential to prolong the QT interval and precipitate cardiac arrhythmias. In 2001, the FDA placed a boxed warning on droperidol that mandated electrocardiogram (EKG) monitoring before and after treatment. This requirement has led to a widespread decrease in use, and the FDA decision sparked significant controversy among clinicians, with many organizations arguing that the evidence did not support this mandate.1
Further review of the cases cited by the FDA revealed that there were 277 reported cases of droperidol-related adverse events (AEs), but many of these cases were duplicates and occurred outside the US.3 Additionally, the doses of droperidol used in these cases were significantly higher than the typical doses used in the emergency department (ED), ranging from 25 to 250 mg.4 Typical doses for PONV range from 0.625 to 2.5 mg intravenous (IV) or intramuscular (IM). Recommended doses for agitation typically range from 2.5 to 10 mg IV and 5 to 10 mg IM.5
There has been growing interest in reevaluating the risk-benefit profile of droperidol in the ED. Since the original decision by the FDA, multiple publications have challenged the idea that droperidol has significantly higher risks associated with its use. The 2014 review by the Clinical Guidelines Committee of the American Academy of Emergency Medicine did not find evidence that low-dose droperidol (< 2.5 is unsafe for use in the ED.6 A retrospective cohort study from 2020 found no fatalities in 5784 patients. Furthermore, a prospective observational study of 1009 patients at 6 EDs who received high-dose droperidol (≤ 20.0 mg) found no evidence of increased risk for QT prolongation.7 The evidence supports the safety of droperidol for use in prehospital and hospital settings as well as in pediatric, adult, and geriatric populations.8-14 Droperidol was eventually reintroduced in 2019, which led to increased use.
The US Department of Veterans Affairs (VA) formulary has limited options (eg, haloperidol and olanzapine) that have robust evidence supporting their use to treat aggression or psychosis-related agitation. Ziprasidone injections are not on the formulary and require authorization for use, which may delay patient care and pose a safety risk. In 2021, VA Greater Los Angeles Healthcare System (VAGLAHS) received Pharmacy and Therapeutics Committee approval to use droperidol in the ED for agitation or nausea and vomiting. The purpose of this study was to evaluate safety outcomes for patients prescribed droperidol and the need for rescue medications (ie, effectiveness) in the VAGLAHS ED.
Methods
This retrospective chart review analyzed patients administered droperidol in the VAGLAHS ED from February 1, 2021, through April 30, 2023. A list of patients who had droperidol ordered in the VAGLAHS ED was obtained from the Veterans Health Information Systems and Technology Architecture. Charts were reviewed using the Computerized Patient Record System to confirm droperidol administration. Nurse documentation was reviewed to confirm the time, dose, and route of administration. In addition, droperidol dosages were categorized as < 5 mg, 5 to 10 mg, and > 10 mg to review outcomes based on the total amount administered to each patient.
Patients included in the study received droperidol in the ED within the study period, were aged ≥ 18 years, and received droperidol for acute agitation or antiemesis. Patients were excluded if they received droperidol for an indication other than agitation or antiemesis.
The study team reviewed the list of patients and audited the collected data. Reviewers were trained on the study protocols and variables identified. The following data were collected: patient demographics (age, sex, race, height, weight, allergies), Charlson Comorbidity Index (CCI) conditions, cardiac comorbidities, laboratory values at admission, basic metabolic panels, liver function tests, droperidol use (doses, indications, and documentation of safety), concomitant medications ordered with the initial droperidol order, AEs (arrhythmias, extrapyramidal symptoms [EPS], respiratory depression, mortality), medications used within 60 minutes of droperidol administration (rescue medications), other medications used within 24 hours after droperidol administration, and EKG/QTc (corrected QT interval) intervals. The data reviewed and recorded were from the date of the initial patient ED visit.
Outcomes
The primary outcome was all-cause mortality within 24 hours after droperidol administration. This outcome was measured in all patients included in this study. Secondary outcomes included rescue medications needed after droperidol administration, incidence of QT prolongation, incidence of EPS (defined as akathisia, dystonia, parkinsonism, or tardive dyskinesia), and incidence of respiratory depression. Clinically significant QTc was defined as an interval of ≥ 500 ms with incidence of arrhythmias, code blues, or intubations. Baseline risk factors for QTc prolongation were taken into consideration including electrolyte abnormalities, concomitant QT-prolonging medications, CCI score, and cardiac comorbidities. Incidence of EPS was counted if patients received medications such as diphenhydramine or benztropine after droperidol administration in addition to documentation of EPS signs and symptoms. Incidences of EPS findings were reviewed by emergency department physicians to confirm the diagnosis.
Safety was assessed by quantifying mortality rates 24 hours after droperidol administration along with incidence of AEs associated with droperidol use including QT prolongation, EPS, and respiratory depression.
The necessity of rescue medication use was assessed by nursing documentation, additional medications ordered, and/or no additional medications required for agitation within 60 minutes of droperidol administration. Sixty minutes was the chosen timeframe given that the onset of droperidol action is between 3 and 10 minutes and peaks in about 30 minutes. Medications that were considered rescue medications included diphenhydramine < 25 mg, diphenhydramine 25 to 50 mg, lorazepam < 1 mg, lorazepam 1 to 2 mg, diphenhydramine < 25 mg and lorazepam < 1 mg, diphenhydramine < 25 mg and lorazepam 1 to 2 mg, diphenhydramine 25 to 50 mg and lorazepam 1 to 2 mg, and other medications, the names and doses of which were manually documented by investigators.
Statistical Analysis
For all variables in the study, descriptive analysis was used to categorize findings. Microsoft Excel was used to calculate means, frequency counts, percentages, and categorize data.
Results
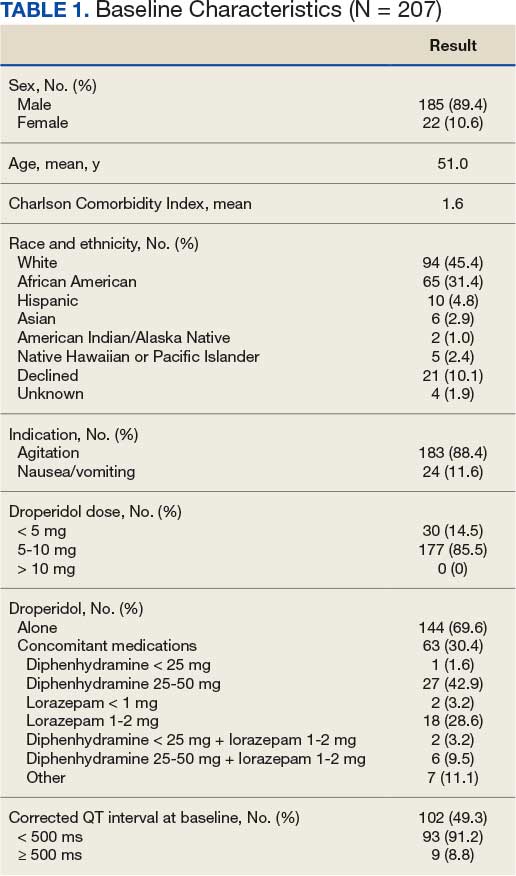
Between February 1, 2021, and April 16, 2023, 214 patients received droperidol in the VAGLAHS ED, and 207 patients were included in the study. Seven patients did not receive droperidol for the indications included (acute agitation or antiemesis). Most of the study population (89.4%) was male, and the mean age was 51.0 years. The mean CCI was 1.6. In the study, 183 (88.4%) patients received droperidol for agitation and 24 (11.6%) for nausea and vomiting (Table 1).
Primary Outcome
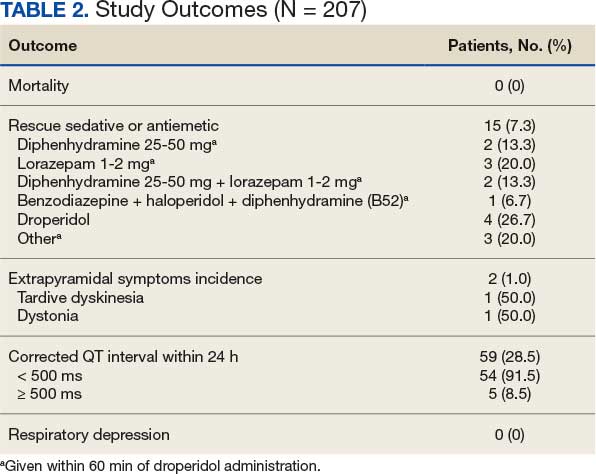
No deaths were observed in a 24-hour period after droperidol administration among the 207 patients included in the study. There were also no arrhythmias, code blues, or intubations observed with the administration of droperidol (Table 2).
Secondary Outcomes
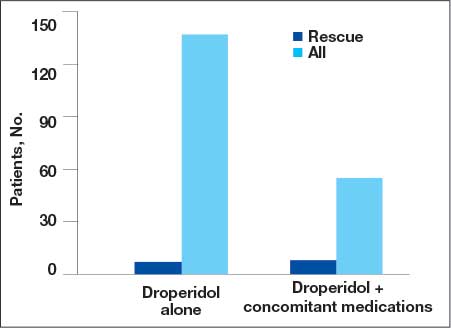
A total of 144 patients (69.6%) received droperidol alone to resolve agitation or nausea and vomiting. In the remaining population, 63 (30.4%) patients were given medications concomitantly with droperidol.
Fifteen patients (7.2%) required rescue medications that were administered within 60 minutes of droperidol administration. Rescue medications were required for 7 patients (4.9%) who initially received droperidol alone compared with 8 patients (12.7%) who were administered concomitant medications with droperidol (Figure).
Extrapyramidal Symptoms
EPS occurred in 2 patients (1.0%). There was 1 incidence of tardive dyskinesia (TD) in which the patient received droperidol 2.5 mg IM for emesis. TD was resolved with diphenhydramine 50 mg. A second patient who experienced dystonia received droperidol 10 mg IM for agitation. Dystonia was resolved with benztropine 2 mg. Both patients had a CCI of 0, no cardiac comorbidities, and laboratory test results were within reference ranges. The second patient received olanzapine within 24 hours of droperidol administration; however, it was after the EPS event.
QTc Prolongation
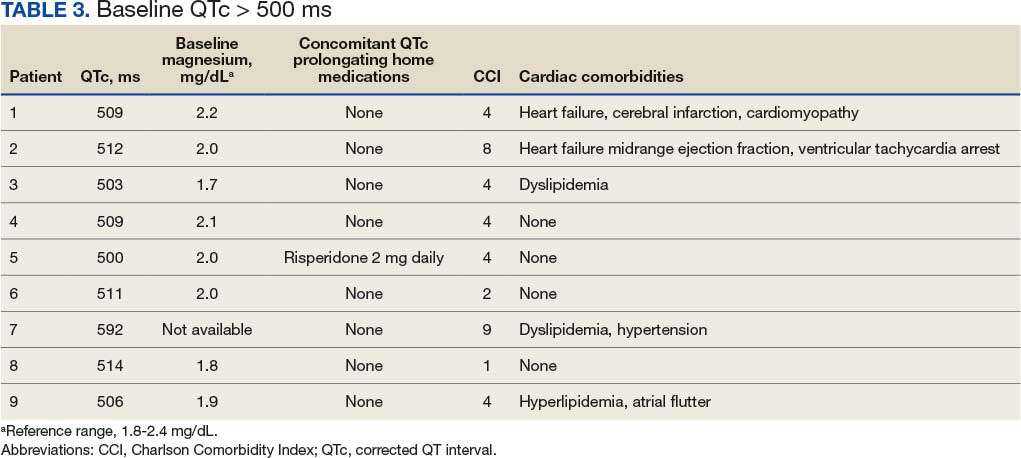
Baseline EKGs (within 6 months prior to ED visit) were available for 102 patients (49.3%). Nine patients (8.8%) had a reported baseline QTc of ≥ 500 ms (Table 3). Of these patients, 6 had a repeat EKG and 5 had a repeat QTc < 500 ms. One patient had a baseline and repeated QTc of 512 ms with essentially no change after droperidol administration. Only 1 patient was on a potentially QTc-prolonging medication at home. None of the patients with baseline QTc > 500 ms experienced arrhythmias after droperidol administration.
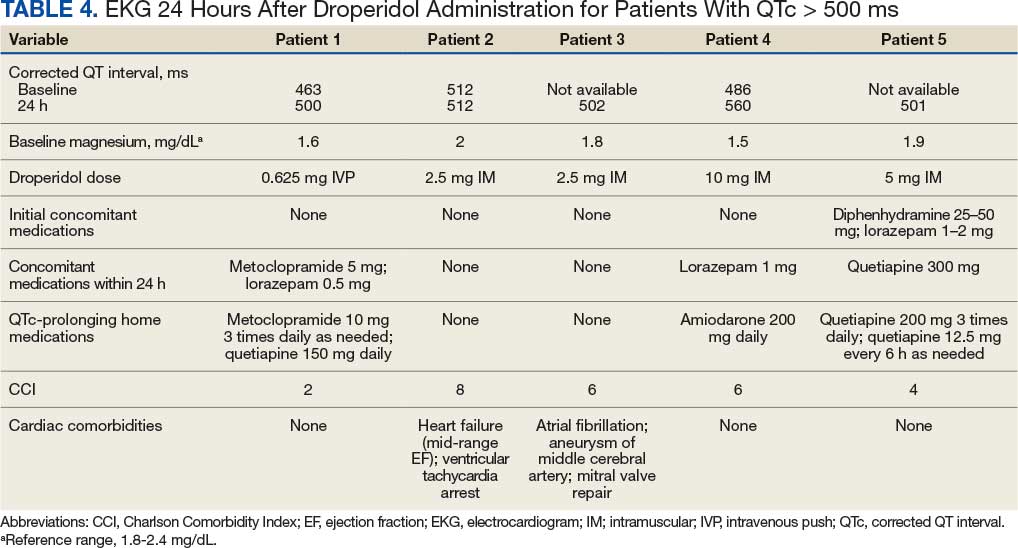
We found that 59 patients (28.5%) had EKGs performed within 24 hours after droperidol administration. Five patients had documented QTc ≥ 500 ms, but no arrhythmias were observed in a 24-hour period. Table 4 describes the additional medications administered after the 60-minute window but within 24 hours after droperidol administration. Quetiapine 300 mg and metoclopramide 5 mg were the only medications documented that can potentially increase QTc. Patient adherence to home medications and the timing of the last dose prior to ED visit were unknown. However, no arrhythmias were noted in these patients with QTc changes. No patients experienced respiratory depression within 24 hours of droperidol administration.
Older Adult Patients
Thirty-eight patients were aged ≥ 65 years with a mean age of 74.2 years. Thirty-four patients (89.5%) received droperidol for agitation and 4 (10.6%) for nausea and vomiting. Only 21 patients had a baseline EKG, and 4 had QTc ≤ 500 ms. At 24 hours, EKGs were performed for 18 patients and 3 had a QTc ≤ 500 ms. No mortality or arrhythmias were reported and there were no incidences of rescue medications, EPS, or respiratory depression.
Discussion
The study included 207 patients who received droperidol for either agitation or nausea/vomiting in the VAGLAHS ED. No mortality occurred within 24 hours of droperidol administration, which is consistent with recent studies.8-14
Furthermore, 59 patients (28.5%) had an EKG performed within 24 hours of droperidol administration; 5 patients had documented QTc ≥ 500 ms. Only 3 of the patients with prolonged QTc had baseline readings for comparison. Only 2 patients had an increase in QTc interval. No arrhythmias were observed; however, the effects of observing QTc prolongation were limited due to the lack of post-EKG readings following droperidol administration. Because of the retrospective nature of the study, neither standardization of EKG at baseline nor 24-hour postadministration were possible. The study found that droperidol was effective with only 15 patients (7.3%) requiring rescue medications. In the patients who were given medications concomitantly with droperidol, it was not possible to conclude whether the patients would have required rescue medications to resolve their agitation or nausea/vomiting. Administration of concomitant medications with droperidol may be attributed to practice patterns associated with haloperidol use, which is frequently administered with concomitant medications such as diphenhydramine and/or a benzodiazepine.
AEs were rare with no documentation of respiratory depression and 2 cases (1.0%) of EPS. Both incidences of EPS resolved with diphenhydramine or benztropine. However, given the reliance on nursing documentation to capture AEs, the number of events may have been underreported.
Limitations
Standardization of dosing was a limiting factor that could affect the need for rescue medications. Another limitation was reliance on nursing reports of resolution of symptoms and comfort with agitated patients. Given the retrospective design and small sample size, this study may not have captured all potential AEs. However, the doses administered within this study population were consistent with what was expected based on other studies.8-14
Conclusions
Droperidol, an antipsychotic, is currently approved for PONV, but is also used off-label for agitation. This study found no fatalities among patients who received droperidol in the ED. The findings suggest that droperidol used for agitation and as an antiemetic, despite its FDA boxed warning, appears to be safe and showed no evidence of mortality, arrhythmias, code blues, or intubations despite the lack of postdose EKG monitoring. Among the 38 patients aged ≥ 65 years, the use of droperidol revealed no increased risks. It should be noted that droperidol appeared safe and few patients required rescue medications within this study population.