Implementation of a Pharmacist-Managed Transitions of Care Tool





Purpose: To improve, expand, and sustain a pharmacist-based transitions of care (TOC) program and to assess interventions targeting veterans at high risk for adverse outcomes.
Methods: A TOC program was developed and piloted at the Richard L. Roudebush Veterans Affairs Medical Center (RLRVAMC). Following success of the pilot project, targeted interventions were identified to improve and expand the program. Patients deemed high risk for readmission by an acute care pharmacist were identified and referred for continued postdischarge follow-up. The study population included patients discharged to the community with primary care established within the RLRVAMC system. Eligible patients were entered into a TOC database by the referring acute care pharmacist. A pharmacist in the primary care clinic reviewed then contacted the patient within 1 week of discharge. Appropriate documentation of each visit was completed in the electronic health record. Data collection included background information, time to follow-up, medication discrepancies, pharmacist interventions, emergency department visits, and hospital readmissions.
Results: A total of 139 patients were included, of which 99 patients were reached for pharmacist follow-up. There were 43 medication-related discrepancies among all patients. The most common discrepancy was taking the wrong dose of a prescribed medication. Additional counseling was provided to 75% of patients. The subset of patients who were reached by a pharmacist had decreased index (5.1% vs 15.0%; P = .049) and all-cause readmissions (8.1% vs 27.5%; P = .03) at 30 days compared with those who did not received pharmacist follow-up, respectively.
Conclusions: This study demonstrated that implementation and expansion of a pharmacist-based TOC process is effective in communicating high-risk patients and intervening on medication-related issues postdischarge.
Primary care services are provided by patient aligned care teams (PACTs), multidisciplinary teams composed of physicians, advanced practice nurses, pharmacists, mental health care providers, registered nurses, dieticians, and care coordinators. Ambulatory Care or PACT clinical pharmacists are established within each RLRVAMC PACT clinic and provide comprehensive care management through an independent scope of practice for several chronic diseases, including hypertension, type 2 diabetes mellitus (T2DM), dyslipidemia, hypothyroidism, and tobacco cessation. Prior to this project implementation, there was no formalized or standardized method for facilitating routine communication of patients between acute care and PACT pharmacists in the TOC process.
Pilot Study
In 2017, RLRVAMC implemented a TOC pharmacy program pilot. A pharmacy resident and both acute care and PACT clinical pharmacy specialists (CPSs) developed the service. The pilot program was conducted from September 1, 2017 to March 1, 2018. The initial phase consisted of the development of an electronic TOC tool to standardize communication between acute care and PACT pharmacists. The TOC tool was created on a secure site accessible only to pharmacy personnel and not part of the formal medical record. (Figure 1).
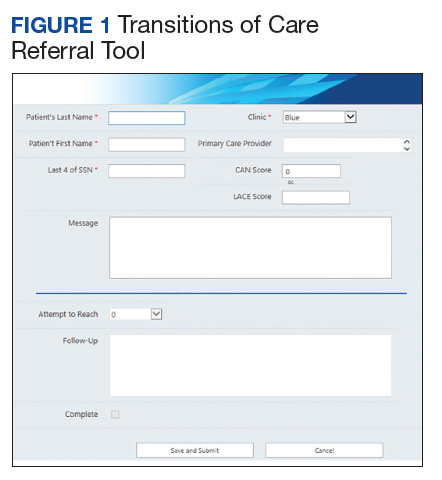
The acute care pharmacist identified high-risk patients through calculated CAN and LACE scores during the discharge process and offered PACT pharmacist follow-up to the patient during bedside discharge counseling. Information was then entered into the TOC tool, including patient identifiers and a message with specific information outlining the reason for referral. PACT pharmacists routinely reviewed the tool and attempted to phone each patient within 7 days of discharge. Follow-up included medication reconciliation and chronic disease management as warranted at the discretion of the PACT pharmacist. All postdischarge follow-up appointments were created and documented in the electronic health record. A retrospective chart review was completed on patients who were entered into the TOC tool.
Patients were eligible for referral if they were discharged during the study period with primary care established in one of the facility’s PACT clinics. Additionally, patients had to meet ≥ 1 of the following criteria, deeming them a high risk for readmission: LACE score ≥ 10, CAN score ≥ 90th percentile, or be considered high risk based on the discretion of the acute care pharmacist. Patients were included in the analysis if they met the CAN or LACE score requirement. Patients were excluded if they received primary care from a site other than a RLRVAMC PACT clinic. This included non-VA primary care, home-based primary care, or VA community-based outpatient clinics (CBOCs). Patients also were excluded if they required further institutional care postdischarge (ie, subacute rehabilitation, extended care facility, etc), discharged to hospice, or against medical advice.
The average referral rate per month during the pilot study was 19 patients, with 113 total referrals during the 6-month study period. Lower rates of index emergency department (ED) visits (5.3% vs 23.3%) and readmissions (1% vs 6.7%) were seen in the group of patients who received PACT pharmacist follow-up postdischarge compared with those who did not. Additionally, PACT pharmacists were able to make > 120 interventions, averaging 1.7 interventions per patient. Of note, these results were not statistically analyzed and were assessed as observational data to determine whether the program had the potential to be impactful. The results of the pilot study demonstrated positive outcomes associated with having a pharmacist-based TOC process and led to the desire for further development and implementation of the TOC program at the RLRVAMC. These positive results prompted a second phase project to address barriers, make improvements, and ensure sustainability.