MODULE 2: Rethinking the Role of Thiazide-Type Diuretics in the Management of Hypertension: Which Diuretic Is Best?






FIGURE 1
Proportion of visits by drug class among patients with drug-treated hypertension11
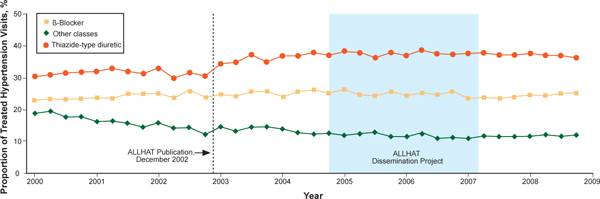
Data are from the IMS Health National Disease and Therapeutic Index, 2000 through 2008. “Other classes” indicates α-adrenergic receptor blockers, potassium-sparing diuretics, loop diuretics, and centrally acting agents.
Source: Archives of Internal Medicine by American Medical Association. Reproduced with permission of American Medical Association, in the format Journal via Copyright Clearance Center.
Hydrochlorothiazide and chlorthalidone: Similarities and differences
Underuse of thiazide-type diuretics is just 1 challenge. Others include which diuretic to use (HCTZ or CTD) and at what dosage.13-17 These 2 diuretics were approved at about the same time and, until recently, were considered equivalent and interchangeable despite differences in structure, pharmacokinetics, and pharmacodynamics.16,17
The publication of the VA Cooperative Morbidity Trial, the successful marketing and popularity of HCTZ and low-dose HCTZ/triamterene, the fear of hypokalemia (which was seen more often in the high doses of CTD initially used), and the subsequent inclusion of HCTZ as the primary diuretic in single-pill combination antihypertensives with ACEIs and angiotensin II receptor blockers (ARBs) led to HCTZ becoming the market leader for this class. Nonetheless, CTD was the diuretic chosen for many major randomized clinical trials, especially those sponsored by the National Heart, Lung, and Blood Institute (NHLBI).5,6,18-20
One reason for CTD’s relegation as a second-tier option to HCTZ could be the higher risk of hypokalemia observed at the higher dosages typically used in early studies.21-23 However, later studies found that substantially lower dosages of CTD could provide similar BP reductions with a significantly lower risk of hypokalemia.24 Materson et al,25 for instance, demonstrated that the 25-mg dosage of CTD was at least as effective for hypertension as the 50-mg and 75-mg dosages, while the 25-mg dosage was associated with less hypokalemia.
Increasingly, however, hypertension specialists, particularly those involved in research, have come to appreciate that CTD and HCTZ are, indeed, not interchangeable and do not have dosing equivalency. This understanding, together with the results of clinical trials like ALLHAT, has led to a resurgence of interest in the use of CTD.17,19,26
One assessment of outpatient prescription data from the VA from 2003 to 2008 found that although the proportion of patients receiving HCTZ during the period remained stable, the number of new users dropped 30% even as the proportion of thiazide users receiving CTD prescriptions doubled from 1.1% to 2.4% and the number of new prescriptions for CTD increased 40%.19
Chlorthalidone or hydrochlorothiazide: Study outcomes
The resurgence of interest in CTD has come with the publication of trials demonstrating its benefits in reducing CVD risk.5,6,27,28
The Multiple Risk Factor Intervention Trial (MRFIT) is the only large, long-term, randomized trial to directly compare HCTZ and CTD, although not in a randomized assignment. The primary endpoint was cardiovascular (CV) outcomes. The study launched in 1973 and enrolled 12,866 males aged 35 to 57 years who were in the upper 15% risk of death from chronic heart disease.29 Participants in the special care group were given HCTZ or CTD (investigator’s choice) at either 50 or 100 mg daily, depending on weight and sodium levels, and were given additional drugs as needed. The control group received usual care at that time from their health care provider. A 44% higher rate of CHD mortality in the HCTZ group observed towards the latter part of the trial led its Policy Advisory Board to change the option between the 2 diuretics and require CTD only. Following the change, the rate of CHD mortality decreased by 28% (P = .04 for comparison between the 2 time frames).29
A recent retrospective analysis of MRFIT found significantly lower CV event rates in participants who received either CTD or HCTZ than in those receiving neither (CTD: adjusted hazard ratio [aHR], 0.51; 95% confidence interval [CI], 0.43-0.61; P < .0001; HCTZ: aHR, 0.65; 95% CI, 0.55- 0.75; P < .0001), but rates of nonfatal CV events were significantly lower in participants who received CTD than those who received HCTZ (aHR, 0.79; 95% CI, 0.68-0.92; P < .0016).30 The results are depicted in FIGURE 2.30
FIGURE 2
Adjusted event-free probability of cardiovascular events30
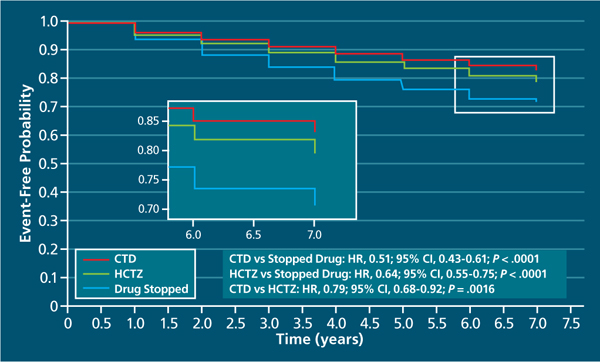
CI, confidence interval; CTD, chlorthalidone; HCTZ, hydrochlorothiazide; HR, hazard ratio.
Source: Hypertension by American Heart Association; Council for High Blood Pressure Research (American Heart Association); InterAmerican Society of Hypertension. Reproduced with permission of Lippincott Williams & Wilkins in the format Journal via Copyright Clearance Center.A recent meta-analysis of 108 trials with HCTZ and 29 with CTD found that the 2 drugs did not provide equivalent reductions in systolic BP (SBP) within equivalent dosages. The study found that the median change in SBP with the median dose of HCTZ was –17 mm Hg, compared with -26 mm Hg for CTD. The slightly greater potassium loss observed with CTD was still nearly equivalent to that observed with HCTZ.31