‘I’m as ugly as the elephant man’: How to recognize and treat body dysmorphic disorder





Body dysmorphic disorder is a common and severe psychiatric malady that often masquerades as other disorders and is usually missed in clinical practice. If recognized and treated appropriately, a majority of patients will improve.
Which psychopharmaceuticals should you consider?
Although BDD’s response to pharmacotherapy has received far less investigation than that of many other psychiatric disorders, research on this treatment approach has dramatically increased in recent years. The following strategies are suggested on the basis of evidence from controlled studies, open-label trials, and the author’s clinical experience (Figure 1):2,6,8,12-17
‘I’m as ugly as the elephant man’

Chris is a shy, anxious-appearing, 31-year-old man who was hospitalized after attempting suicide. He wears a baseball cap pulled down over his forehead and partially covering his eyes. It is difficult for him to reveal the reason for his suicide attempt: “It’s really hard to talk about this. I don’t know if I can. It’s too embarrassing.” Then he adds, “Well I guess I should tell you—after all, I’m in the hospital because of it. It’s my nose—these huge pock marks on my nose. They’re grotesque! I look like a monster. I’m as ugly as the elephant man!
“These marks on my nose are all I can think about. I’ve thought about them for hours a day every day for the past 15 years. I even have nightmares about them. And I think that everyone can see them and that they laugh at me because of them. That’s why I wear this hat all the time. And that’s why I couldn’t talk to you in a bright room. You’d notice the marks and see how ugly I am.” Chris actually appeared entirely normal, but no one could convince him of this.
“This has affected me in a lot of ways,” Chris adds. “This may be hard for you to believe, but this problem has ruined my life. All I can think about is my face, and I spend hours a day looking at the marks in the mirror. I just can’t resist. I thought I looked so ugly that I started missing more and more work, and I stopped going out with my friends and my girlfriend. I got so anxious when people looked at me that I started staying in the house most of the time. Sometimes when I did go out, I went through red lights so I wouldn’t have to sit at the light, where people might be staring at me. The hat helped a little, but it didn’t cover all the marks. I tried covering them with makeup for a while, but I thought people could see the makeup so that didn’t really help. The only time I really felt comfortable is when I wore my nephew’s Batman mask on Halloween—then no one could see the marks.
I finally missed so much work that I was fired. My girlfriend stuck it out with me for a long time, but finally she couldn’t take it any more. One thing that was really hard for her was that I started asking her about 50 times a day whether I looked OK and whether she could see the marks—I think that was the final straw. If I had a choice, I’d rather have cancer. It must be less painful. This is like an arrow through my heart.”
Chris had a notable, although only partial, response to fluoxetine 100 mg/d and buspirone 60 mg/d (higher doses of fluoxetine and buspirone were tried but were not more effective). Adding clonazepam was helpful for severe anxiety. Clomipramine, venlafaxine, lithium, mirtazapine, and various antipsychotics were sequentially added to this regimen, with minimal success, although a second trial of olanzapine, at a higher dose (15 mg/d) than he had been willing to try previously, further decreased Chris’ BDD and depressive symptoms. The addition of bupropion was somewhat helpful for depression but not for BDD.
Figure 1 Proposed pharmacotherapy for treating BDD
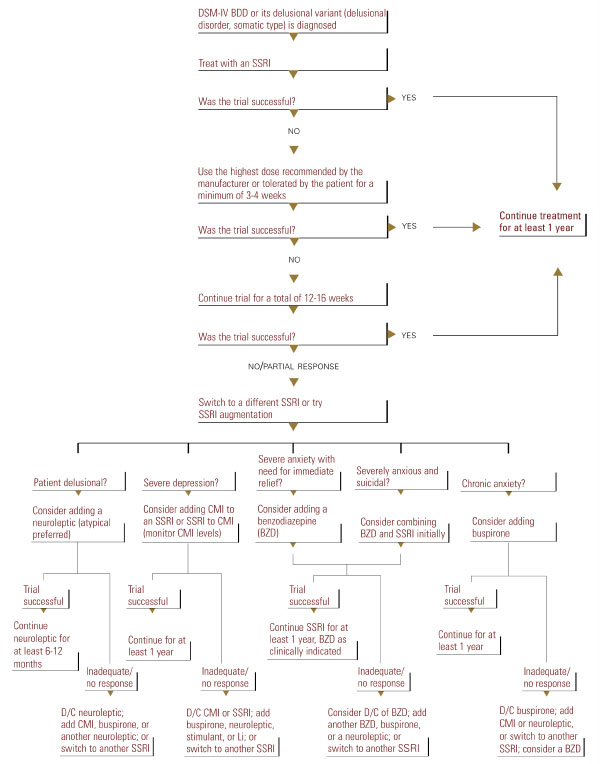
- Use an SSRI as a first-line approach. Other medications, including other antidepressants, appear less effective than SSRIs or clomipramine.2,8,9,13,15 An SSRI or clomipramine is also recommended for patients with delusional BDD (those who are completely convinced that they look abnormal and cannot be convinced otherwise), as Proposed pharmacotherapy for treating BDD these patients appear to respond to SSRIs as well as nondelusional patients do.12-17
- Use the maximum recommended or tolerated SSRI dose if lower doses are ineffective. Although no studies have compared different SSRI dosages, BDD appears to often require higher doses than those that are typically used for depression.
In a chart-review study of 90 patients with BDD treated in the author’s clinical practice, the mean SSRI doses used were fluoxetine 66.7 ±23.5 mg/d, fluvoxamine 308.3 ±49.2 mg/d, paroxetine 55.0 ± 12.9 mg/d, sertraline 202.1 ± 45.8 mg/d, and clomipramine 203.3 ±52.5 mg/d.17 Some patients respond only to doses higher than the maximum recommended dose (for example, 80-100 mg/d of citalopram or paroxetine).