Psychiatrist/patient boundaries: When it’s OK to stretch the line





Some boundary crossings are therapeutic, but beware the ‘slippery slope’ to violations.
Glass uses a Venn diagram to illustrate that although most boundary crossings probably fall within the realm of ethical practice, gray areas alert therapists that they are approaching a violation (Figure).20 Five factors have been found to increase psychiatrists’ vulnerability to boundary violations (Table 1).22
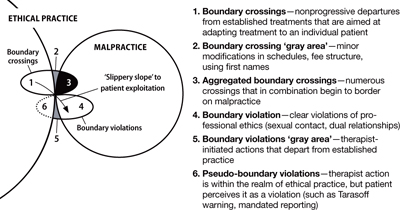
Figure Beware the ‘gray areas’ between boundary crossings, violations
Source: Glass L. The gray areas of boundary crossings and violations. Am J Psychother 2003;57(4):429-44. Republished with permission of the Association for the Advancement of PsychotherapyTable 1
Boundary violations: Factors that increase your vulnerability
| Life crises—effects of aging, career disappointments, unfulfilled hopes, or marital conflicts |
| Transitions—job changes or job loss |
| Medical illness |
| Arrogance—the belief that a boundary violation couldn’t happen to you and not recognizing the need for consultation |
| Stress points shared by the patient |
| Source: Reference 22 |
CASE CONTINUED: Board investigation
Dr. M’s relationship with Ms. Y grows intense, and he becomes increasingly concerned about her “clinginess.” After several months, Dr. M feels emotionally suffocated and ends the relationship. Despondent and suicidal, she seeks treatment in the local emergency room. Ms. Y tells the ER psychiatrist about her relationship with Dr. M and that she cannot go on without him in her life. The ER psychiatrist refers her to another psychiatrist for outpatient care, and, with Ms. Y’s permission, files a complaint about Dr. M with the state medical board and the district branch ethics committee.
The state medical board investigates Dr. M. He is contrite about his actions and their effect on Ms. Y. The state board refers Dr. M to an impaired physician’s program. He is required to attend a boundary violations course and undergo 1 year of practice supervision by a local psychiatrist. Several years later, Dr. M is doing well in his practice and has had no further complaints lodged against him.
Boundaries vs relationships. Using boundaries as a metaphor for maintaining the separation of therapist and patient was intended to serve the analytic process and to protect the patient’s welfare.2 Clearly, certain boundaries—such as sexual contact between psychiatrist and patient—must remain sacrosanct. Yet certain practices avoided in analysis may be appropriate for other therapeutic interventions. For example, whereas psychoanalysis has strict prohibitions against seeing patients anywhere except in the office, cognitive-behavioral therapists may find it useful to conduct sessions in public, or—under carefully arranged circumstances—even in a patient’s home. Other examples include accompanying a patient with agoraphobia to a public gathering or dining with a patient with anorexia.
Exercise caution when you decide to alter traditional boundaries. Even minor crossings that are not likely to progress to violations have the potential to contaminate the therapeutic relationship and place the psychiatrist on a “slippery slope” to patient exploitation.22,23 Some boundary issues are ambiguous, and extenuating circumstances can create a context that temporarily stretches a boundary beyond its normal limits,24 especially in small communities and rural settings where patients and treating psychiatrists are likely to know and encounter each other in social settings.25 Our recommendations for avoiding boundary violations appear in Table 2.
Except in clear cases of malfeasance, determining whether or not you have crossed a boundary is not a straightforward decision based on a single theoretical perspective or absolute standard.26 Regardless of whether a given boundary’s edge is well defined, 2 things are clear:
- unlike patients, psychiatrists have a professional code to honor27
- harm is determined by the meaning of the behavior to the patient and not the psychiatrist’s intentions.4
Table 2
Simple steps help avoid boundary violations
| Dos |
| Know your state’s statutes regarding medical ethics |
| Stay abreast of the American Psychiatric Association’s Principles of Medical Ethics |
| Consult with colleagues |
| Be aware of your weaknesses |
| Avoid ‘slippery slopes’ |
| Use objective documentation |
| Build a satisfying personal life |
| Don’ts |
| Don’t foster dependency |
| Don’t use patients for your own gratification |
| Don’t engage in extra-therapeutic contacts |
| Avoid physical contact |
| Don’t accept gifts or services |
Related Resources
- American Medical Association. Principles of medical ethics. www.ama-assn.org/ama/pub/category/2512.html.
- American Psychiatric Association. The principles of medical ethics with annotations especially applicable to psychiatry. Washington, DC: American Psychiatric Association; 2008.
Disclosures
Drs. Marshall and Myers report no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
Dr. Teston is a speaker for Shire US, Inc.