Antidepressants for bipolar depression: Tips to stay out of trouble





When it makes sense to use them and for how long.
Table 1
Switches vs destabilization: Defining antidepressant risks
| Risk | Definition |
|---|---|
| Acute switches to hypomania/mania | ≤8 weeks by convention, unless dosage is increased |
| Mood destabilization | |
| Cycle acceleration | Increase of ≥2 mood episodes while taking antidepressants, compared with a similar exposure time before treatment |
| Rapid cycling | ≥4mood episodes in previous 12 months (new-onset or exacerbation of baseline pattern), according to DSM-IV-TR |
| Source: Reference 1 | |
Switching risk. Some researchers have reported antidepressant-induced switches to be milder and more brief than spontaneous hypo/manias,13 whereas others have observed more-severe mixed14 and even psychotic episodes. Risk factors that may predispose patients to switching include:
- personal or family history of switches or mood destabilization
- family history of bipolar disorder
- exposure to multiple antidepressant trials
- history of substance abuse or dependence
- early onset (age <25) and/or treatment of mood symptoms.15,16
True switch rates are difficult to estimate because clinical trials have used different switching definitions, durations, antidepressants (with or without mood stabilizers, and with different mood stabilizers), and cohorts (often excluding rapid cyclers). Except for the Nemeroff et al study,6 no prospective, double-blind, placebo-controlled studies have examined switch rates, and even this study was not large enough to detect statistically significant differences.
Thus we must rely on naturalistic evidence that is less rigorous but more applicable to clinical practice. This literature reveals switch rates of:
- 30% to 60% with TCAs and monoamine oxidase inhibitors (MAOIs)
- 15% to 27% with selective serotonin reuptake inhibitors (SSRIs), bupropion, and venlafaxine.
Average switch rates are thought to be approximately 40% with TCAs/MAOIs and 20% with the newer antidepressants.1 Preliminary data associate venlafaxine with higher switch rates than SSRIs or bupropion, so perhaps antidepressants with some noradrenergic effects (including TCAs) facilitate the switching phenomenon.17
Mood destabilization. Three randomized, controlled trials suggest that antidepressants—especially TCAs—increase the risk of cycle acceleration or rapid cycling in bipolar patients. The best designed study—sponsored by the National Institute of Mental Health—was a 10-year, prospective, double-blind trial of 51 rapid-cycling patients. The trial’s on-off-on design showed that 20% of these patients developed rapid cycling as a direct result of taking TCAs.18
Unfortunately, most randomized, controlled trials are not designed to show a relationship between antidepressants and mood destabilization. Observational literature is mixed but suggests that antidepressant use is associated with rapid cycling. Most evidence supports a relationship between antidepressants and long-term mood destabilization—especially cycle acceleration, which is believed to occur in approximately 20% of patients using TCAs or SSRIs.1
Are mood stabilizers protective? Some studies suggest that mood stabilizers may help protect against switches. Most of the evidence—using lithium and TCAs—suggests a 50% drop in switch rates when patients receive mood stabilizers with antidepressants. In one study, lithium was more protective than anticonvulsants for SSRI-induced mania, but the difference was not statistically significant.19
Because study data variability, we don’t know if some mood stabilizers are more effective than others in preventing antidepressant-related switching. This variability is likely caused by:
- medication-specific factors (such as higher switch rates with TCAs and possibly dual-reuptake inhibitors than with SSRIs)
- illness-specific factors (such as rapid cycling and cycle pattern)
- patient-specific factors, already described. Mood stabilizers appear to be more protective against switching than against mood destabilization, in which their effects are less clear (Table 2).15
Table 2
Frequency of switching or mood destabilization with antidepressants
| Bipolar risk | Causative agents | Frequency | Mood stabilizer effect |
|---|---|---|---|
| Acute switch | TCAs, MAOIs | ~ 40% | Variably protective; apparent partial risk reduction ~ 50% |
| SSRIs, bupropion, venlafaxine | ~ 20% | ||
| Mood destabilization | TCAs, SSRIs | ~ 20% | Not as clearly protective against mood destabilization as against acute switching |
| TCAs: tricyclic antidepressants; MAOIs: monoamine oxidase inhibitors; SSRIs: selective serotonin reuptake inhibitors | |||
| Source: References 1, 15 | |||
TREATMENT RECOMMENDATIONS
How does a clinician decide which bipolar depressed patients should receive antidepressants?
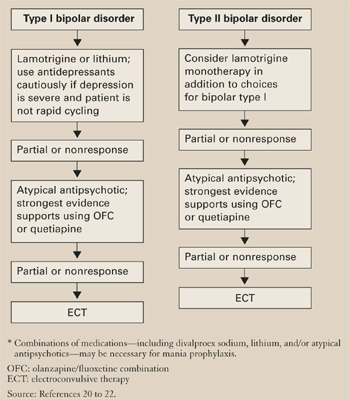
The first step in treating bipolar depression (Algorithm) is to provide optimal dosages of the patient’s mood stabilizers. Consensus guidelines20 suggest lithium or lamotrigine as first-line treatments for bipolar depression. Evidence also shows efficacy for atypical antipsychotics, including the olanzapine/fluoxetine combination (OFC)—FDA-approved for acute bipolar depression21—and quetiapine monotherapy.22 Dosages vary, but suggested ranges include:
- lithium: 0.6 to 1.2 mEq/L; aim for approximately 0.8 mEq/L, but some data suggest 0.6 to 0.7 mEq/L may be sufficient
- lamotrigine: 50 to 250 mg/d (the higher dosage is based on maintenance studies)
- OFC: 6 to 12 mg olanzapine/25 to 50 mg fluoxetine
- quetiapine: 300 to 600 mg/d.
The next step is an antidepressant risk/benefit analysis, weighing the considerable risks of switching/mood destabilization with the patient’s depressive illness severity, type of bipolar disorder (such as rapid cycling), and cycle pattern.
Algorithm Recommended treatment of bipolar depression
Cycle patterns. In a naturalistic study, Macqueen et al23 used life chart data for 42 bipolar patients to assess how the mood state preceding a prospectively observed depressive episode affected treatment response: