New Investigators: What makes aripiprazole the ‘different’ antipsychotic





Off-label use of ‘dopamine stabilizer’ requires caution.
Aripiprazole’s intrinsic activity allows for higher D2 receptor occupancy with fewer side effects associated with full dopamine receptor antagonism. Clinical implications of this profile are unknown. Dopamine’s role in schizophrenia’s pathophysiology is inferred from knowledge that all effective antipsychotics offer some postsynaptic D2 receptor blockade.
Conventional dopamine receptor agonists (DAs) such as haloperidol and the newer serotonin-dopamine receptor agonists (SDAs) modeled after clozapine are thought to exert clinical effect by blocking D2 and D3 receptors. By contrast, partial dopamine agonists are agonists or antagonists, depending on cell-specific, synaptic dopamine concentrations. DAs and SDAs are competitive, full antagonists at pre- and postsynaptic dopamine receptors, whereas partial dopamine agonists are:
- agonists at presynaptic regulatory autoreceptors and in hypodopaminergic (mesocortical) synapses
- antagonists with small intrinsic activity in hyperdopaminergic (mesolimbic) synapses. Intrinsic activity is a compound’s degree of agonism in proportion to full agonism.
‘Dopamine stabilizers.’ Because of this combination of high-affinity receptor antagonism with preserved intrinsic activity, some call partial dopamine agonists “dopamine stabilizers.”
Source: References 11, 12
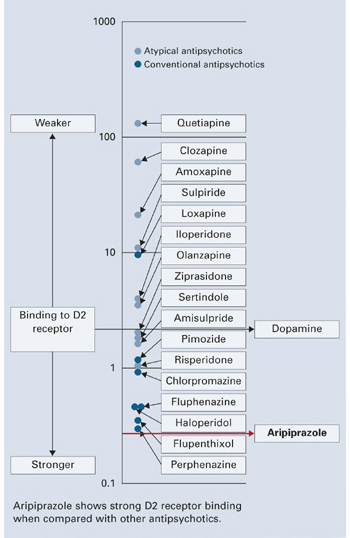
FigureAntipsychotics’ D2 receptor binding affinities
SIDE EFFECTS
Evidence shows fewer side effects with aripiprazole when used to treat schizophrenia and schizoaffective disorder compared with DAs such as haloperidol and SDAs such as risperidone.1,2,4
Dosage-dependent somnolence occurs with aripiprazole; the most common side effects include headache, agitation, anxiety, and insomnia (24.5%, 34.6%, 24%, and 18.6%, respectively).2 continued on page 60 A 10-week, placebo-controlled study using aripiprazole, 2 to 15 mg/d, to treat psychosis in Alzheimer’s dementia showed significantly increased risk of somnolence, accidental injury, and bronchitis (likely caused by aspiration).16
In placebo-controlled trials, aripiprazole, 2 to 30 mg/d, did not increase risk of cardiac, lipid, or prolactin-related side effects2 but showed increased risk of:
- tremor when used at 15 mg/d for up to 26 weeks in chronic schizophrenia, (9% incidence vs 1% with placebo)17
- akathisia when used at mean dosages of 27.9 mg/d to treat acute bipolar mania (11% incidence vs 2%with placebo).3 Aripiprazole also increased akathisia incidence in normal subjects.18
Risk of tardive dyskinesia or hyperglycemia-related adverse events with aripiprazole are unknown. Studies report weight gain of <1 kg (<2.2 lbs) in patients taking aripiprazole, 2 to 30 mg/d. One study found that patients switched from DA and SDA antipsychotics to aripiprazole, 30 mg/d, lost on average 1.5 kg (3.2 lbs) across 8weeks.19
Determining neuroleptic malignant syndrome risk with aripiprazole is difficult; two cases were reported in the premarketing sample.16 One animal study showed diminished catalepsy with chronic aripiprazole use, in contrast to persistent catalepsy with haloperidol.20
A Medline search for aripiprazole in February 2005 found several reports of treatment-emergent side effects, including:
- 3 reports of worsening agitation or psychosis21-23
- 2 reports of EPS24,25
- 1 report of excessive somnolence in a child.26
Adverse effects are probably underrepresented. Clinical deterioration and adverse effects were reported after starting, switching to, or combining aripiprazole with other antipsychotics or serotonergic agents (trazodone, sertraline, or venlafaxine).27,28
This paper by Dr. Mahendra T. Bhati was entered in the 2005 Promising New Investigators competition sponsored by the Neuroleptic Malignant Syndrome Information Service (NMSIS). The theme of this year’s scholarly papers was “New insights on psychotropic drug safety and side effects.”
Current Psychiatry is honored to publish this peer-reviewed, evidence-based article on a clinically important topic for practicing psychiatrists.
NMSIS is dedicated to reducing morbidity and mortality of NMS by improving medical and psychiatric care of patients with heat-related disorders; providing support information for medical professionals, patients and families; and improving scientific understanding of these conditions through research.
Related resources
- Lieberman, J. Aripiprazole. In: Schatzberg, A, Nemeroff, C (eds.) Textbook of Psychopharmacology. Washington DC: American Psychiatric Publishing, 2004:487-494.
- FDA Center for Drug Evaluation and Research. https://www.fda.gov/cder/foi/nda/2002/21-436_Abilify.htm
- Medline Plus Drug Information. https://www.nlm.nih.gov/medlineplus/druginfo/medmaster/a603012.html
Drug brand names
- Aripiprazole •Abilify
- Clozapine • Clozaril
- Haloperidol • Haldol
- Risperidone • Risperdal
- Trazodone • Desyrel
- Sertraline • Zoloft
- Venlafaxine • Effexor
Disclosure
This author is supported by grant 2R25MH060490-06 from the National Institute of Mental Health.