Hypothyroidism: Clinical Challenges in Diagnosis and Treatment





Although accreditation for this CE/CME activity has expired, and the posttest is no longer available, you can still read the full article.
Expires July 31, 2015
–
Although hypothyroidism is common, its typically vague symptoms of fatigue, lack of energy, and weight gain are shared with many other conditions. Awareness of risk factors for hypothyroidism will aid in the differential diagnosis, and the patient’s symptoms can help guide the clinician to the appropriate diagnostic workup. Thyroid function test results are necessary to confirm or rule out the diagnosis.
LABORATORY WORKUP
Thyrotropin
The diagnosis of hypothyroidism is based on the results of the TSH test, which is the primary screening test for thyroid dysfunction.4 TSH secretion is extremely sensitive to minor increases and decreases in T3 or T4, making it the most reliable laboratory test for the assessment of thyroid function. An elevated serum TSH level in the presence of hypothyroid symptoms is diagnostic of primary hypothyroidism. Other causes of elevated TSH, such as thyrotropin-secreting pituitary tumors, are rare, and their symptomatology is different.3
Free Levorotatory Thyroxine
Though elevated TSH levels occur before T4 abnormalities are detected, T4 measurement can sometimes be useful in the diagnosis of hypothyroidism, especially in cases of possible central hypothyroidism. As a diagnostic test, measurement of serum free T4 (FT4) is preferable to total T4 because T4 binds to specific proteins in serum, making obtaining an accurate total T4 level subject to factors that alter binding. By contrast, FT4, the metabolically active form of the hormone, is not affected by binding factors. In primary hypothyroidism, FT4 is low or normal.4
Measurement of the FT4 level will also confirm the diagnosis of central hypothyroidism, if the FT4 is low when TSH is normal or low. As FT4 decreases, the TSH should elevate to compensate; in the presence of a low FT4, even a normal TSH is indicative of hypothyroidism. In a patient with overt hypothyroid symptoms with a normal TSH, an FT4 should be ordered for further workup.4
Triiodothyronine
Measurement of the serum T3 level, whether total or free, is of little clinical utility because it often remains normal, even as TSH and T4 levels change.4
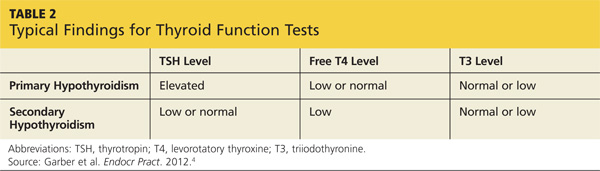
Typical diagnostic test results in primary and secondary hypothyroidism are summarized in Table 2.
Other Factors That May Affect Thyroid Function Test Results
The overall health status of the patient must be considered when evaluating the results of thyroid function tests because the results can be affected by other factors.
• Serum TSH may be low, often in combination with low FT4, in hospitalized patients with acute illness.
• TSH may increase to levels above normal during recovery from nonthyroid-related illness.
• Serum TSH typically falls (infrequently to below 0.1 mlU/L) during the first trimester of pregnancy due to the stimulatory effects of human chorionic gonadotropin on the thyroid.5 Levels typically return to normal in the second trimester.
• TSH and FT4 can be altered in the postpartum period secondary to postpartum thyroiditis. Levels will often resolve on their own without treatment.
• Patients with anorexia nervosa may have low TSH levels as well as low levels of FT4 secondary to pituitary and hypothalamic dysfunction.
• Mild TSH elevations may also be a normal manifestation of aging; TSH values above 3.0 mlU/L occur with increasing frequency with age.4
Thyroid Peroxidase Antibodies
Testing the patient for thyroid peroxidase (TPO) antibodies, although not required to make the hypothyroidism diagnosis, may provide additional useful information. A positive TPO antibody result is significantly associated with hypothyroidism; in particular, TPO antibodies are more likely to be present in patients with autoimmune thyroiditis, helping to confirm the diagnosis.2,4 However, positive antibody test results do not change clinical management decisions. Results will remain positive during treatment, and the continued presence of antibodies warrants no alteration in treatment or medication dose.
An elevated TPO antibody level does impart a risk for future transition to overt hypothyroidism, so this test is recommended for patients with subclinical hypothyroidism. In addition, for patients with other autoimmune diseases, such as type 1 diabetes or Addison disease, or with chromosomal disorders, such as Down or Turner syndromes, TPO antibodies suggest a propensity toward hypothyroidism. Current research also indicates that both pregnancy rates and pregnancy outcomes improve when TPO antibody–positive patients whose TSH levels are above 2.5 mlU/L are treated.5
On the next page: Diagnosis and treatment >>