Hypothyroidism: Clinical Challenges in Diagnosis and Treatment





Although accreditation for this CE/CME activity has expired, and the posttest is no longer available, you can still read the full article.
Expires July 31, 2015
–
Although hypothyroidism is common, its typically vague symptoms of fatigue, lack of energy, and weight gain are shared with many other conditions. Awareness of risk factors for hypothyroidism will aid in the differential diagnosis, and the patient’s symptoms can help guide the clinician to the appropriate diagnostic workup. Thyroid function test results are necessary to confirm or rule out the diagnosis.
Although hypothyroidism is common, its typically vague symptoms of fatigue, lack of energy, and weight gain are shared with many other conditions. Awareness of risk factors for hypothyroidism will aid in the differential diagnosis, and the patient’s symptoms can help guide the clinician to the appropriate diagnostic workup. Thyroid function test results are necessary to confirm or rule out the diagnosis.
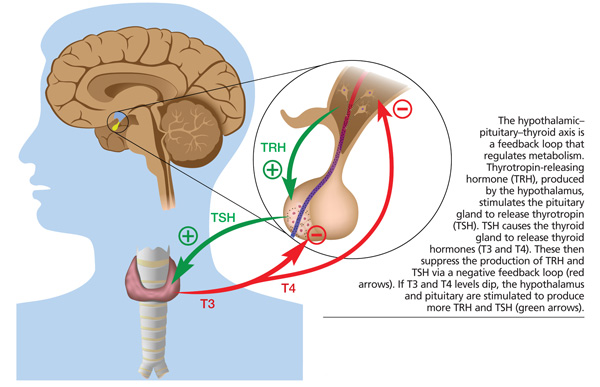
Approximately 4.6% of the US population ages 12 and older has been diagnosed with hypothyroidism, making it the most frequently diagnosed thyroid disorder.1 Hypothyroidism is defined by an underproduction of thyroid hormones and can be either primary or secondary. Primary hypothyroidism is caused by the failure of the thyroid gland to produce adequate quantities of the hormones triiodothyronine (T3) and levorotatory thyroxine (T4). Secondary (central) hypothyroidism is a result of inadequate production of thyrotropin (TSH) by the pituitary gland; less often, it is caused by inadequate production of thyrotropin-releasing hormone by the hypothalamus. The great majority of patients with hypothyroidism have the primary form of the disease. In the US, the most common cause of
hypothyroidism is chronic autoimmune thyroiditis (Hashimoto thyroiditis); worldwide, it is iodine deficiency.
Because hypothyroid symptoms are vague, the disease can be difficult to diagnose. Patients most often present with complaints of fatigue and lack of energy, raising suspicion for hypothyroidism; but true symptomatic, overt hypothyroidism is rather rare, occurring in only 0.3% of the population.2
Subclinical hypothyroidism, in which TSH levels are elevated but T3 and T4 levels are normal and the patient experiences few, if any, symptoms, is much more common. This makes the use of diagnostic laboratory tests essential; hypothyroidism cannot be diagnosed based on clinical presentation alone. Signs and symptoms may include fatigue, lack of energy, cold intolerance, weight gain, thinning hair/hair loss, dry skin, constipation, menstrual cycle abnormalities, irritability, and depression. Bradycardia and hypotension are also possible. Physical examination may reveal depressed affect, eyelid edema, loss of lateral third of the eyebrow, thickened tongue, dry skin, and hyporeflexivity; however, most patients will have a benign and unrevealing physical examination.3
Hypothyroidism is more common in white people and in women and increases in incidence after age 60. Risk factors for hypothyroidism include
• Family history
• Autoimmune disorders (eg, type 1 diabetes, Addison disease)
• History of Graves disease treated with radioactive iodine or thyroidectomy
• Past external beam radiotherapy for head and neck malignancies
• Postpartum thyroiditis
• Turner and Down syndromes
• Multiple sclerosis
• Amiodarone or lithium use
• Iodine deficiency or previous residence in an iodine-deficient area.4
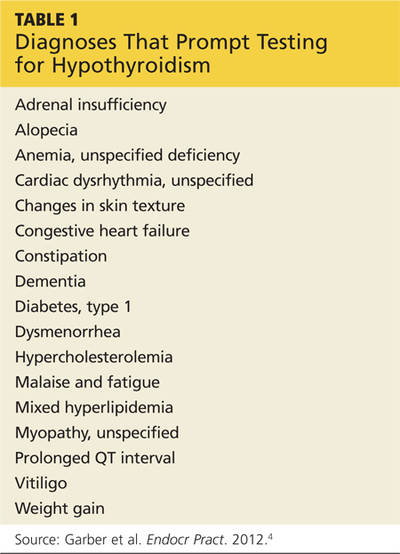
In addition, testing for hypothyroidism may be warranted in patients with any of the diagnoses in Table 1.
Because of its vague symptomatology, hypothyroidism can mimic many disease processes. However, the most pertinent include depression, anemia, and dementia/Alzheimer disease. Laboratory testing will almost always identify hypothyroidism.
On the next page: Laboratory workup >>