
A practical approach to vestibulitis and vulvodynia






Draw a few basic distinctions and apply simple strategies to aid your diagnosis and management of these all-too-common conditions
IN THIS ARTICLE
Evaluation can be tricky
The key to evaluation of a patient with these complaints is to schedule her appointment once she has been off therapy for at least 2 weeks and has not used any intravaginal medication during that interval. This drug holiday serves two functions:
- It eliminates adverse reactions to medications from the differential diagnosis.
- It allows adequate evaluation of vaginal secretions, including a reliable vaginal culture for Candida species.
During this initial encounter, the exam may well be normal. Ask the patient to grade her vulvovaginal symptoms on a scale of 0 to 10, with 10 representing the worst symptoms experienced and 0 being a complete lack of symptoms. Many patients at the initial encounter will grade their symptoms as minimal, in the range of 2 to 3 out of 10.
If the exam is normal, ask the patient to return for a repeat evaluation when her symptoms reach 8 or greater on the 10-point scale, and instruct her not to self-treat with a topical or systemic antimicrobial. When she returns, vulvovaginal candidiasis can usually be diagnosed by microscopy and confirmed by vaginal yeast culture to rule out non-albicans Candida. Patients who have recurrent vulvovaginal candidiasis tend to flare premenstrually.
Treatment may be lengthy
Treatment of cyclic vulvovaginal candidiasis involves an initial course of oral fluconazole (150 mg every 3 days for three doses), followed by suppressive therapy with weekly fluconazole (150 mg).2 This treatment is effective in more than 90% of cases, easing the cyclicity of the patient’s symptoms. However, she may be left with some residual vestibulitis and discomfort with coitus, which may take as long as 2 months to resolve. Biweekly application of a topical steroid of modest strength may help, such as triamcinalone 0.1% ointment.
Vestibulitis is most common among young women
Women who have vestibulitis tend to be premenopausal and young—typically, in their 20s. They usually complain of worsening pain with coitus, as well as pain with tampon insertion and tenderness when riding a bike or wearing tight jeans, suggesting that touch to the vestibule provokes the pain.
Despite these other symptoms, however, it is the inability to have vaginal sexual intercourse that usually brings the patient to the physician. I generally ask a simple question: “If you did not engage in sexual intercourse, would you be normal?” In other words, would she avoid the pain if she avoided touch to the vestibule? Patients who have vestibulitis inevitably answer, “Yes!”
“The eye doesn’t see what the mind doesn’t know”
This caveat is important as you examine the patient (FIGURE 1). When vestibulitis is present, clinical findings are often subtle; careful examination, however, can elicit the source of the tenderness. Inspect the vulvar vestibule carefully circumferentially, and exert pressure at the junction of the hymen and vestibule using a moistened cotton swab.
As I mentioned earlier, women who have vestibulitis have evidence of focal erythema and, sometimes, focal erosion at the junction of the hymen and vestibule. They also experience exquisite tenderness as the cotton swab presses against this junction, with the pain most intense in the 3 to 9 o’clock region. Yeast vaginitis should be ruled out by microscopy and yeast culture.
Most patients have avoided coitus for some time before they see a physician, so vestibular fissures may not be obvious. The diagnosis of vestibulitis can be based on Friedrich’s criteria:
- severe pain at the vestibule upon touch or attempted vaginal entry
- tenderness to pressure localized within the vulvar vestibule
- physical findings confined to vestibular erythema of various degrees.3
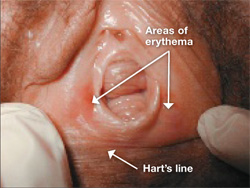
FIGURE 1 Physical findings may be subtle
When vestibulitis is suspected, look for areas of erythema or fissuring at the junction of the hymen and vestibule and explore the entire vestibule out to Hart’s line.
Medical therapy is ineffective
Vestibulitis is a disease that renders the vestibular epithelium less resilient and more susceptible to fissures upon contact. For this reason, medical therapy is ineffective.
Although a 6-week trial of a topical steroid (triamcinalone 0.1% or desoximetasone 0.25% ointment twice daily) is commonly prescribed, it is rare for a patient to have a response sufficient to restore pain-free coitus.4
Some patients are adept at applying topical 5% xylocaine ointment to the vestibule 15 to 30 minutes before coitus to ease the discomfort associated with intercourse. Another alternative is injection of interferon into the vestibule, which can limit the percentage of patients who require vestibulectomy by almost 50%. However, interferon must be injected into the vestibule three times weekly for 4 weeks.5 Side effects include the pain of the needlestick and systemic fever and flu-like illness from the interferon.
