Permanent contraception provides a lesson in cost-effective medicine







Moving interval sterilization into the office, using the hysteroscope, appears to benefit patients and society—a good thing in 2010
Some women, who have completed their family strongly prefer a tubal sterilization over an IUD. For them, selecting a cost-effective method is important:
- For a woman who is planning a repeat cesarean delivery and not to have more children afterward, tubal ligation can be performed at delivery with little additional cost
- Tubal sterilization following vaginal delivery is also an efficient approach in many clinical settings; this might be especially true in populations that have a high risk of pregnancy between the time of delivery and initiation of an effective contraceptive postpartum
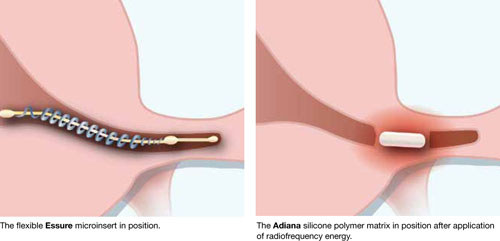
- Approximately 50% of women who choose tubal sterilization will not have the procedure at the time of delivery; they elect an interval procedure. These women must choose between an office-based procedure such as hysteroscopic tubal sterilization, using either the Adiana or the Essure method (FIGURE), or an in-hospital procedure such as laparoscopic tubal ligation.
FIGURE Two methods of in-office hysteroscopic tubal sterilization
Comparing the office hysteroscopic procedure and in-hospital laparoscopic tubal ligation
For any given condition, most procedures performed in a hospital are more costly than procedures that can be performed in a physician’s office. A hospital is, after all, a high-cost environment, in part because it has multiple missions, including providing free care and 24-hour emergency services. What the literature shows. Several cost-effectiveness studies have concluded that office-based hysteroscopic tubal sterilization is more cost-effective than in-hospital laparoscopic tubal ligation:
- In three studies that compared Essure hysteroscopic tubal sterilization performed in an office and laparoscopic tubal ligation performed in a hospital day-surgery unit, investigators concluded that Essure sterilization was 33% to 60% less expensive6-8
- In a fourth study, both aforementioned procedures were performed in a non-hospital ambulatory center; there, Essure was determined to be 10% less expensive than laparoscopic tubal ligation9
- Others have also concluded that hysteroscopic sterilization is cost-effective, especially when performed in an office.10
There is less published information available about the comparative costs of Adiana hysteroscopic tubal sterilization and laparoscopic tubal ligation; Adiana was approved for use by the FDA only last year. It is likely, however, that Adiana also offers a cost advantage over in-hospital laparoscopic tubal sterilization.
Cost-effectiveness analyses never perfectly mirror the real world
It’s difficult to account for all costs associated with an intervention (TABLE). For example, some studies have reported that patients recover more quickly, and fully, after hysteroscopic sterilization than after laparoscopic tubal ligation.11 Most studies of tubal sterilization do not account for patient and employer costs involved in recovering from a laparoscopic sterilization procedure.
Another challenge is calculating the cost incurred by the patient as she waits 3 months for a hysteroscopic procedure to achieve contraceptive effectiveness. After laparoscopic tubal sterilization, contraceptive effectiveness is established immediately; after hysteroscopic sterilization, another form of contraception must be used for 3 months before hysterosalpingography is performed to document successful tubal occlusion. The cost to the patient of waiting 3 months is seldom included in cost-effectiveness analyses—in part because it is hard to quantify that wait in dollars.
TABLE
Some characteristics of Essure and Adiana may affect their relative* cost
| Essure | Adiana | |
|---|---|---|
| Method | A microinsert comprising 1) an inner coil of stainless steel and polyethylene terephthalate fibers and 2) an outer coil of nickel titanium is placed in the interstitial portion of each fallopian tube by means of hysteroscopy | A delivery catheter is placed in the tubal ostium. The tip of the catheter contains an electrode array that can deliver thermal injury when activated. After the thermal event, a silicone implant is released into the tube. |
| Follow-up | Hysterosalpingography is used to assess successful tubal occlusion approximately 3 months after the procedure. Before successful occlusion is demonstrated, the patient should use another form of contraception. | |
| Additional equipment | None | Requires a device-specific radiofrequency generator to induce thermal damage |
| *Relative to each other and to other methods of contraception. SOURCE: Palmer SN, Greenberg JA. Transcervical sterilization: a comparison of Essure permanent birth control system and Adiana permanent contraception system. Rev Obstet Gynecol. 2009;2(2):84–92. | ||
How we practice must address the need to trim costs
Under the new law, widened access to health care will trigger an intense focus on reducing costs. The delivery of health care will need to change, in many ways, to ensure that the interventions we use are the most cost-effective ones. Office hysteroscopic tubal sterilization may be one cost-cutting measure that benefits both the individual patient and greater society.
INSTANT POLL
What are your preferred methods of tubal sterilization?