Can safety and efficacy go hand in hand? Contraception for medically complex patients






There may be more options than you think for women who have one or more medical conditions
IN THIS ARTICLE
Interval sterilization with laparoscopic tubal ligation is usually performed with general anesthesia. The rate of major morbidity is approximately 0.9%, including major bleeding, need for laparotomy, organ injury, and major infection. Complications may be higher in women with diabetes, a history of major surgery, and obesity.28
The WHO advises caution when using this method in the setting of severe diabetes, sickle cell disease, coagulopathy, severe renal disease, cardiovascular disease, or pulmonary disease.1
Insertion of intratubal coils is less invasive than tubal ligation
Hysteroscopic tubal sterilization with placement of titanium–Dacron intratubal coils (sold by the name Essure) is another option gaining use (FIGURE). Although large-scale studies have yet to be published, data from the largest phase III trial are consistent with smaller studies.29 In that multicenter trial, coil placement was successful in 92% of patients, and 99% of women completed the procedure without general anesthesia. Tubal perforation was identified in 1% of women, who went on to a laparoscopic procedure.
This less invasive method of permanent sterilization increases options for women who are poor laparoscopy candidates, although the 10% of women who experience technical failure will be forced to find an alternative method. Patient compliance is also an issue because the woman must use backup contraception for 3 months following the procedure, until tubal occlusion is confirmed by hysterosalpingography.
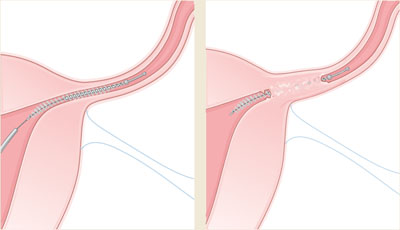
FIGURE Sterilization via insertion of intratubal coils
Delivery of the Essure device.
After 3 months, polyethylene (PET) fibers elicit ingrowth and proximal tubal occlusion.
Focusing on the patient’s partner may be the smartest approach
Male sterilization with vasectomy poses no medical risks to a woman with a complex medical history. However, long-term success requires that she keep the same sexual partner throughout her reproductive life or seek another form of contraception.
CASE RESOLVED Patient opts for progestin-only pills
Because of her sickle cell disease, D.M., the patient described at the beginning of this article, is not a good candidate for surgical sterilization, and neither is her boyfriend. According to WHO criteria, her sickle cell disease falls into category 2 in regard to combined OCs and category 1 for IUC—both effective methods. No guidance is available regarding concomitant use of steroids, which she is taking for lupus, with IUC, but her baseline risk for pelvic infection is thought to be relatively low. The noncontraceptive benefit of ovarian cyst suppression makes combined OCs even more attractive for this patient, but her history of stroke contraindicates this method (category 4). Depot medroxyprogesterone acetate may suppress ovarian function and is classified as category 3. She ultimately selects a combination of progestin-only pills and condoms and has successfully avoided pregnancy.