How to overcome a resistant cervix for hysteroscopy and endometrial biopsy






A cervix that impedes access to the uterus can lead to severe pain, cervical laceration, and other ills
IN THIS ARTICLE
Is stenosis present? Stenosis is most common in nulliparous and postmenopausal women and in those who have undergone cervical procedures such as cryotherapy. Stenosis increases the risk of laceration and uterine perforation.
Consider a mechanical dilator. When cervical dilation is difficult, a series of small Hagar or lacrimal duct dilators may be helpful (FIGURE).
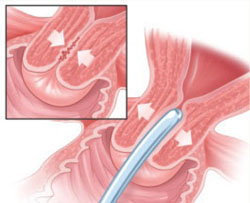
FIGURE Mechanical dilation is one antidote to cervical stenosis
In challenging cases, such as cervical stenosis, mechanical dilation with a series of Hagar or lacrimal duct dilators may facilitate entry into the cervix.
Pain can be mild—or it can thwart your work
Although many women tolerate placement of a small hysteroscope without analgesia or anesthesia, pain and vasovagal reaction sometimes occur. Indeed, the level of pain experienced by the patient is a major determinant of the overall success of the procedure.3,8-10 Pain can occur when a tenaculum is used to grasp the anterior cervix, as well as during cervical dilation, injection of local anesthetic, or insertion of the hysteroscope. In some cases, a smaller scope may be all that is needed to solve the problem.11
Analgesia may not always be necessary
Some researchers have studied office hysteroscopy without analgesia or anesthesia, finding a high level of acceptance.12,13 Others have found a significant percentage of women requesting anesthesia or analgesia (16.5%)10 or requiring local anesthesia (28.8%).8
Preoperative NSAIDs may suffice. Use of oral nonsteroidal anti-inflammatory drugs (NSAIDs) 1 hour before office hysteroscopy may reduce intraoperative and postoperative pain.7 Nagele and colleagues8 compared use of mefenamic acid 1 hour before the procedure with placebo in 95 women undergoing outpatient diagnostic hysteroscopy. Mefenamic acid reduced pain at 30 and 60 minutes after—but not during—the procedure. Other studies have found that pain is reduced when an oral NSAID is taken 1 to 2 hours before insertion of an intrauterine device and before suction curettage.14,15
Other perioperative medications may help reduce discomfort and patient anxiety, including anxiolytics, such as lorazepam, analgesics, and conscious sedation.3
Paracervical block may be appropriate when pain is very likely
A number of investigators have evaluated use of paracervical anesthesia during out-patient hysteroscopy.9,13,16,17 They injected lignocaine or mepivacaine using a 21- or 22-gauge needle at 3, 5, 7, and 9 o’clock or 4 and 8 o’clock paracervically.13 One study found paracervical block to be effective in reducing the pain of tenaculum placement and insertion of the hysteroscope.17 However, some studies suggested a reduction of pain in postmenopausal women only.9 These women may be more likely to have cervical stenosis.
Paracervical block does pose a risk of complications. Studies have reported bleeding in some women16 and pain with injection of the paracervical block, as well as bradycardia and hypotension possibly secondary to intravascular injection.17
Other methods are inconsistent
Intracervical injection. Some researchers have recommended injection of local anesthetic into the cervix.13 One study found no benefit—in fact, the injection appeared to be the most painful part of the procedure.18 A case series suggested that injection of local anesthetic may be effective, but the series lacked a placebo or control arm.13
Topical intrauterine anesthetic has been investigated after administration through the channel of the hysteroscope or by a catheter passed through the cervix into the uterine cavity.13 Findings have been mixed, with some researchers demonstrating reduced pain19,20 and others showing no relief.21
Topical cervical anesthesia. Some hysteroscopists have recommended application of anesthetic cream, gel, or spray directly to the cervix immediately before the procedure.13,22 The results have been mixed, with some studies noting decreased pain overall,13 one finding decreased pain only during tenaculum placement,22 and others finding no significant reduction in pain any time during the procedure.13,23,24 A review concluded that topical cervical lignocaine spray may reduce the discomfort of tenaculum placement.13
Topical anesthesia may minimize vasovagal reaction
In one study, 1.1% of women undergoing office hysteroscopy experienced a vasovagal reaction, caused by stimulation of the parasympathetic nervous system with cervical manipulation and passage of the scope through the internal os of the cervix.25 The reaction led to hypotension and bradycardia. Several studies have suggested that a local anesthetic can reduce this complication.19,20
Cicinelli and associates found that topical local anesthesia reduced the incidence of vasovagal reaction from 32.5% in the control arm to 5%.20 They suggest that a local anesthetic be considered in selected women, such as postmenopausal patients, who are at increased risk of vasovagal attack.
In contrast, Lau and associates17 found an increased rate of bradycardia and hypotension with paracervical lignocaine (31% versus 10%), but it may have been caused by inadvertent intravascular injection.17
Researchers have also suggested that the use of smaller hysteroscopes may reduce the incidence of vasovagal reactions.26