Diagnosis and safe management of placenta previa






As repeat cesareans increase, so do placental abnormalities
IN THIS ARTICLE
Transvaginal ultrasound is superior for diagnosis of previa
Leerentveld et al20 reported false-positive and false-negative rates of 1% and 2%, respectively—a striking improvement over transabdominal ultrasound, which has rates of 2% to 6% and 7%, respectively.
Transvaginal sonography has several advantages over transabdominal imaging in localization of the placenta. The shorter distance from the vaginal probe transducer to the cervix and lower uterine segment allows the use of higher-frequency ultrasound waves, with improved resolution; therefore, the relationship between the placental edge and the internal os can be determined more accurately.
Some clinicians may worry that the probe used in transvaginal sonography will disrupt the placenta and provoke significant maternal hemorrhage, but this concern is unfounded. Multiple studies have attested to the safety of transvaginal sonography in localization of the placenta.5,20-22 The probe is introduced and positioned under direct ultrasound guidance at all times, and inadvertent insertion of the endovaginal probe into the internal cervical os is virtually impossible due to the anatomical relationship of the vagina and cervix.21
Transperineal ultrasound is another option. Several investigators have found it to be superior to transabdominal and similarly advantageous to transvaginal sonography in the diagnosis and exclusion of placenta previa.18
Start with transabdominal imaging
In current practice, transabdominal ultrasound is usually performed first to localize the placenta. If there is reason to suspect placenta previa, transvaginal or transperineal sonography is then used to confirm the location of the placenta.
Contractions may hinder imaging
Accurate diagnosis or exclusion of placenta previa may be difficult if uterine contractions are present during ultrasound evaluation. Myometrial contractions shorten the distance between the internal cervical os and the placental edge, altering measurement of this distance. In addition, the ultrasound appearance of a contraction may simulate placental tissue, making it difficult to exclude placenta previa.
The trouble with tradition
The 4 types of placenta previa in the traditional classification system—complete, partial, marginal, and low-lying—predate the era of ultrasound diagnosis and are based on digital palpation of the placenta through a partly dilated cervical os during labor.
A new system of 3 types
Along with other authors,5,15-18 we propose a new system with 3 categories—complete, incomplete, and low-lying—because ultrasound may not distinguish a placenta partially covering the internal os (a discrete point) from one that is merely encroaching on it.
Complete previa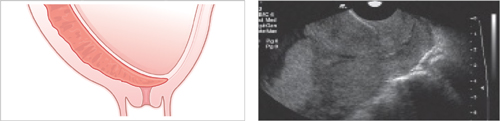
The placenta completely covers the internal cervical os
Incomplete previa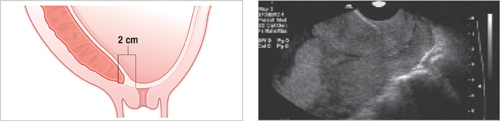
The placental edge is within 2 cm of the internal cervical os, but does not cover the os
Low-lying previa
The distance from the internal cervical os to the placental edge is between 2 and 3.5 cm
Look for placenta accreta
When placenta previa is diagnosed by ultrasound examination, further diagnostic measures are needed to determine whether placenta accreta is present.5,23 In placenta accreta, neither the normal plane of separation between the placental villi and uterine wall, nor the intervening fibrinoid layer of Nitabuch, is present.5,23
Degrees of abnormal placental implantation
Risk of accreta can reach 67%
There are varying reports on the incidence of placenta accreta, but women with placenta previa and previous cesarean deliveries appear to have the highest incidence.3,23,24 In women with placenta previa and 1 previous cesarean section, the risk of placenta accreta has been estimated at 24%, but it increases to 67% for women with placenta previa and 4 previous cesarean sections.3
Sonographic appearance of placenta accreta
Certain characteristics are suggestive of placenta accreta25,26:
Unfortunately, diagnosis of placenta accreta is difficult prior to delivery, although transvaginal sonography and adjunctive color flow/power Doppler imaging with 2- and 3-dimensional techniques offer improved resolution and have yielded promising results in prenatal diagnosis.27-30
Magnetic resonance imaging (MRI) may also prove useful in detecting placental tissue invasion and evaluating the degree of invasion, especially in a posterior or lateral placenta previa or when there is invasion into the bladder.31-33
Gestational age, symptoms determine management
The management of women with placenta previa in the third trimester depends on the extent of maternal hemorrhage and the fetal gestational age. Clinical categories include:
Some asymptomatic cases resolve
Outpatient management is possible for women who have never bled after diagnosis in the second trimester. These women should abstain from intercourse, avoid digital examination after 20 weeks’ gestation, and immediately present to the hospital if there is any evidence of vaginal bleeding.34
Monthly ultrasound evaluations are necessary to determine whether placenta previa has resolved,34-37 since 90% of cases detected in the second trimester resolve by the third trimester.34 However, if placenta previa persists beyond 24 weeks’ gestation, there is a 50% risk that delivery will be complicated by it.35 If placenta previa persists after 32 weeks, that risk approaches 75%.35