Osteopenia: When to intervene?






Why fracture risk assessment should rely on a constellation of factors—not just a numerical bone-density value
Thus, the T score is only part of the story.
Another example: A 38-year-old woman with a long history of poor calcium ingestion and several years of hypomenorrhea in her 20s has a T score of –2. This woman does not have the same fracture risk as a 63-year-old woman who also has a T score of –2, but who had a T score of 0 when she entered menopause at age 49. These 2 women have the same bone mass, but very different levels of bone quality and fracture risk.
So which women should have their bone mass tested?
Various organizations have issued guidelines for measuring BMD in women to assess risk of fracture (TABLE 3).
FIGURE 1 Risk of fracture increases with advancing age and continuous loss of bone
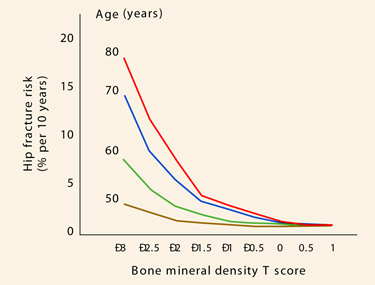
Adapted from Kanis JA, Johnell O, Oden A, Dawson A, De Laet C, Jonsson B. Ten year probabilities of osteoporotic fractures according to BMD and diagnostic thresholds. Osteoporos Int. 2001;12:989–995.TABLE 3
3 sets of guidelines on who needs a bone mineral density test
| ORGANIZATION | CRITERIA |
|---|---|
| National Osteoporosis Foundation2 |
|
| US Preventive Services Task Force3 |
|
| International Society for Clinical Densitometry4 |
|
| NOTE: Per guidelines of the International Society for Clinical Densitometry, women discontinuing estrogen should be considered for bone-density testing according to the indications listed above. | |
When to intervene?
It should be said that it is never too early to intervene when it comes to important lifestyle issues. Adequate calcium and vitamin D are essential throughout life for all women. Encouraging patients to quit smoking is crucial, as is fall prevention, especially for frail women and those with poor eyesight. It is beneficial for women to maintain flexibility, agility, mobility, and strength; these are important components of bone health and total health, and should be taught early in life.
Teriparatide is a bone builder…
This agent is the first parathyroid hormone analog that is anabolic and can build new bone. All the older, familiar agents (estrogen, bisphosphonates, selective estrogen receptor modulators) are antiresorptive. That is, they act by retarding the resorptive part of the dynamic lifelong process whereby bone is constantly laid down and taken away.
…not a magic bullet
When I first heard of anabolic compounds such as teriparatide several years ago, I naively thought it might be possible to modify our approach to bone health. Instead of treating patients to prevent osteoporosis, why not simply wait until patients developed the disease and then treat them with anabolic bone-building agents?
The problem with such reasoning is this: Although the risk of fracture is higher in women with osteoporosis, the number of fractures is greater in postmenopausal women with osteopenia because there are so many more women with osteopenia than with osteoporosis. In fact, the Surgeon General’s report on the state of bone health in the United States estimated that 34 million women have osteopenia and 10 million women have osteoporosis.5
Thus, it becomes obvious that we cannot simply wait until women have developed osteoporosis to treat them if we are going to prevent the majority of fragility fractures.
3 studies exposed risk of osteopenic fracture
The MORE trial
The Multiple Outcomes of Raloxifene Evaluation (MORE) trial6 involved 7,705 women less than 80 years of age in a randomized, placebo-controlled, multicenter, double-blind study of postmenopausal osteoporosis. One of the groups studied had T scores as low as –2.5 and no previous fractures. The other group had 1 or more vertebral fractures at baseline. Women were randomized to raloxifene or placebo for 3 years. Partway through the trial the relevant T-score database was corrected,6 which had the effect of recategorizing many women originally enrolled with “osteoporosis” as “osteopenic.”