Anal sphincter injury at childbirth






Immediate or delayed repair? Overlapping or end-to-end technique? Midline or mediolateral episiotomy? Plus: risk factors, and tactics for subsequent deliveries.
Future pregnancies: Set course by symptoms
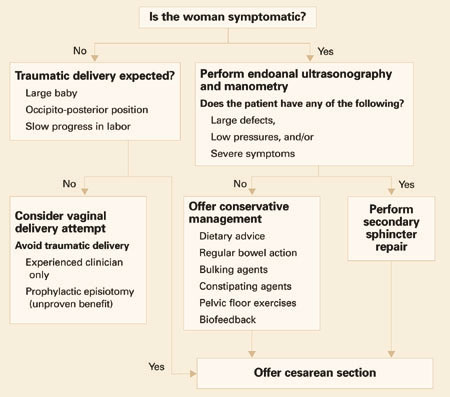
Consider subsequent vaginal delivery only under these circumstances (FIGURE 2):
- The woman is asymptomatic.
- She has no evidence of anal sphincter defects detected by endoanal scan or low pressures on manometry.
- Delivery will be carried out by an experienced midwife or doctor.
Since no evidence suggests that an elective prophylactic episiotomy will prevent another tear, perform episiotomy only if clinically indicated (ie, if the perineum is thick and inelastic, and an episiotomy will prevent multiple radial tears).
Asymptomatic women with low squeeze pressures and a defect greater than 1 quadrant are at increased risk of developing anal incontinence following another vaginal delivery; therefore, counseling should include the option of cesarean section.
Symptomatic women with severe injuries. Offer a secondary sphincter repair, and deliver future pregnancies by cesarean.
Women with mild symptoms can be managed conservatively with:
- dietary advice to avoid gas-producing foods,
- regulation of bowel action,
- bulking agents,
- constipating agents such as loperamide and codeine phosphate,
- pelvic floor exercises, and
- biofeedback.
This group of women is at risk of deterioration with a subsequent vaginal delivery, and should therefore be offered cesarean section. The risk of developing a repeat 3rd-degree tear is low, but no randomized studies have been performed to evaluate the benefit of routine cesarean section.
The author reports no financial relationships relevant to this article.
FIGURE 2 Pregnancy after sphincter injury: How to manage delivery30