Does menopause always justify bone density testing?






Anne has new-onset hot flashes, Beth’s mother broke a hip, Carol thinks she’s not at risk, Donna has 6 risk factors. Is bone density testing appropriate?
The guidelines
The NOF, AACE, the American College of Obstetricians and Gynecologists (ACOG), NAMS and the United States Preventive Services Task Force (USPSTF) guidelines12-14,19,20 agree that all postmenopausal women age 65 and older should have bone density testing. With the exception of the USPSTF, they also agree that all postmenopausal women under age 65 with risk factors should be tested. (The USPSTF limits this recommendation to women age 60 to 64.)
In reality, all postmenopausal women should have bone density testing because the list of risk factors is so comprehensive that it is unusual to find a woman who does not have at least 1 risk factor for osteoporosis.
Anne:Test again in 1 year
With this information in mind, let’s again consider Anne, the 53-year-old woman who sought help for hot flashes. Her visit was an opportunity to discuss osteoporosis prevention. Of the major risk factors, Anne has 2: weight less than 127 lb and a fracture after age 40. Based on the recommendations from the NOF, AACE, ACOG, and NAMS, bone density testing is appropriate.
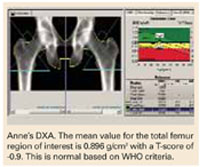
A DXA study of both proximal femurs shows bone density data for each femur individually as well as the mean BMD value for each region of interest for both femurs. There are 5 regions of interest in the proximal femur: the total hip (or total femur), the femoral neck, Wa rd’s area, the trochanter, and the shaft. The total hip or femoral neck is preferred for diagnosis. Based on her normal T-scores, Anne does not meet any of the pharmacologic intervention guidelines. She should nevertheless be counseled on nonpharmacologic interventions to prevent bone loss.
She should have another bone density study in 1 year. Anne’s PA lumbar spine DXA study is not shown, but it provided no additional information. The PA lumbar spine would be the preferred site for follow-up in 1 year, however.
The recommendation for follow-up in 1 year would not change even if you elected to begin low-dose combined-continuous HRT for relief of hot flashes. Although HRT would be expected to preserve her skeleton, follow-up testing in 1 year for confirmation is appropriate.21
Beth:Treat now, test in 1 yr
Beth has an important risk factor: her mother’s hip fracture. This raises the possibility that she is genetically predisposed to lowerthan-average peak bone density. She meets NOF, AACE, NAMS, and ACOG guidelines for bone density testing.
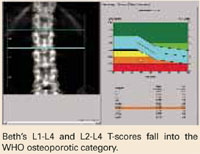
At the PA lumbar spine, it is preferable to use either the L1-L4 BMD or the L2-L4 BMD and the corresponding T-score. In either case, Beth’s T-score is disturbingly low at -3.7 and -3.6, respectively. Either T-score meets the diagnosis of osteoporosis based on WHO criteria.
This single bone density study does not reveal whether she has lost bone density from a previously higher level or whether her current bone density represents her peak bone density. It is incumbent on the physician to evaluate her medically to exclude possible causes of bone loss other than estrogen deficiency, which might require a different or additional therapy.
Beth certainly meets NOF, AACE, and NAMS guidelines for drug intervention.
A follow-up PA lumbar spine DXA study is indicated in 1 year. Although she has osteoporosis, she has not yet had a fracture. For now, her diagnosis is nothing more than a test result. An osteoporotic fracture will change that. Immediate intervention with drug therapy can preserve her skeletal mass and her quality of life.
Donna:Borderline T-scores
Treatment decisions are not always as clear as in the cases of Anne, Beth, and Carol. Consider Donna, age 54, who is 2 years postmenopausal and in good health. However, her mother reportedly had a dowager’s hump at the time of her death. Although Donna was never told that her mother had osteoporosis, you suspect that she did because of the kyphosis. Donna is fairly sedentary, thin, and continues to smoke. She is not using HRT and rarely takes nutritional supplements of any kind. L 1 - L 4 PA lumbar spine T-score is -1.4; total hip is -1.3.
The dilemma is that Donna does not meet any guideline for pharmacologic intervention based on T-score, even in the presence of risk factors. Both T-scores are just above the NOF and AACE cutoff points, even in the presence of risk factors.
But the guidelines are not hard and fast rules. T- score cutoff points, with or without other risk factors, were chosen to balance the potential benefit and any potential harm of pharmacologic therapy with the risk of fracture if untreated. So, while it may seem arbitrary to recommend treatment when the T- score is -1.5 with risk factors, yet not if the T-score is -1.4 or -1.3, there is a substantive rationale behind the recommendation. Still, there is no substitute for your judgment.