Safe delivery of the fetal head during cesarean section






Safely extracting the fetal head from a low station can turn a standard cesarean birth into an arduous procedure. Here the author describes a sequence of maneuvers to resolve the problem while minimizing strain on the incision.
Instead, try 1 of the following 2 approaches: The first option is to extend your arm in a straight line from shoulder to fingertip, keeping it almost parallel to the patient’s longitudinal axis. This is accomplished by flexing forward at the waist while facing cross-table, and abducting your arm out from your shoulder. Another option is to turn and face the head of the table, flex at the waist, and extend your arm behind you while pronating your hand. Both of these positions keep your wrist angle neutral and allow you to use the strength and leverage of your entire upper trunk to move your hand.
In order to elevate the head, your fingers need to achieve at least a quarter-circle grip around the vertex (FIGURE 1). If the head is so deep or tightly applied that you cannot achieve this in 1 continuous movement, proceed in stages. First, have an assistant apply transvaginal digital pressure to elevate the head from below. Then, advance your fingers as far as you can around the fetal head while flexing and extending the fingers in a worm-like wiggling movement. Flex and lock your fingers against the fetal cranium, and lean your entire upper trunk and arm away from the maternal pelvis. This generally elevates the head by roughly a centimeter, enough to advance your fingers a little further. Repeat these motions until your fingers have achieved the desired quarter-circle, at which point your assistant may withdraw from below.
Now lock your arm from shoulder to fingertip, and lean out of the patient’s pelvis 1 more time. You may note the sensation and sound of breaking suction as the fetal head escapes the pelvic grip. Maintain this steady traction for several seconds. When the vertex has reached the level of the lower margin of the uterine incision, you can rotate the fetus.
Rotate. Before you begin rotation, confirm the fetal position (the fetal ears are useful as a landmark). If the head is not already in occiput anterior, grasp it and rotate the occiput into the incision (FIGURE 2). As in vaginal delivery, this presents the shortest fetal-head diameters to the birth orifice. If the head has been markedly molded by labor, rotation will bring the narrow end of a dilating cone into the uterine incision. This helps direct the head anteriorly, rather than back into the pelvis, when fundal pressure is applied.
Reduce. Using your hand like a pair of forceps may cause uterine extensions or lacerations if the uterine incision is not large enough to accommodate both your hand and the fetal head. Instead, use 4 fingers in shoehorn fashion to guide the head out of the incision. First, however, there is usually another obstacle to overcome: Fundal pressure may merely force the head back toward the pelvis. Your fingers cannot present a shallow enough angle to direct the head anteriorly, unless your hand is in so deep that your palm fills the uterine incision.
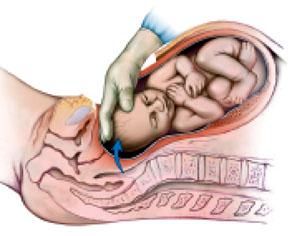
You may substitute instruments for the guiding fingers, using the Murless head extractor, the Torpin vectis blade, or 1 blade of a short-shank Simpson forceps. However, a lack of availability may limit your choices. Although you may use a disposable vacuum extractor system, consider saving that expense with this alternative: Using your fingertips, reduce the lower lip of the uterine incision beneath the fetal head, as you would reduce a posterior cervical lip at a vaginal delivery. (FIGURE 3). The reduced lip tends to extend the head anteriorly and direct it away from the pelvis. Withdraw your hand so only your fingertips remain to guide the head, while the back of your fingers retract the lower abdominal wall. With fundal pressure the head should move anteriorly out of the abdomen.
A head in the occiput-posterior position may resist attempts to rotate to occiput anterior. Should this occur, try following the incision reduction with direct manual flexion of the head out of the abdomen. If reduction flexion puts excess strain on the incision, abandon the attempt. Instead, use a disposable vacuum extractor cup—placed on the fetal brow as close to the vertex as possible—to flex the head out of the incision. Should this fail as well, extend the low-transverse uterine incision cranially into a generous U-incision, and repeat the vacuum procedure.
FIGURE 1 THE ERR SEQUENCE
Elevate. Lock the fingers into a quarter-circle around the vertex. Apply traction out of the pelvis with the hand and the entire extended arm.
FIGURE 2 THE ERR SEQUENCE
