
Heterotopic pregnancy: an emerging diagnostic challenge






Due in part to rising rates of in vitro fertilization, heterotopic pregnancy isn’t nearly as rare a condition as it was in times past. Here, the authors detail protocols for diagnosing and treating this challenging disorder.
An interstitial or cornual pregnancy discovered at surgery may be difficult to distinguish from an angular pregnancy, i.e., an intrauterine pregnancy that implants in the lateral angle of the uterine cavity. The distinction is crucial, however, because an angular pregnancy is more likely to miscarry (38%) than to rupture.6 The angular pregnancies that do not miscarry are more likely to involve preterm labor. Interstitial eccyesis is surgically diagnosed by a hemorrhagic swelling in the uterine cornua that either displaces the round ligament anteriorly or the ovarian ligament posteriorly, depending upon whether it erodes through the anterior or posterior walls of the tube, respectively (FIGURES 2 and 3).7 An angular pregnancy appears as a similar cornual swelling, but does not distort the anatomical relationships between the round or ovarian ligaments and the fallopian tube.
FIGURE 1 Anatomy of the fallopian tube
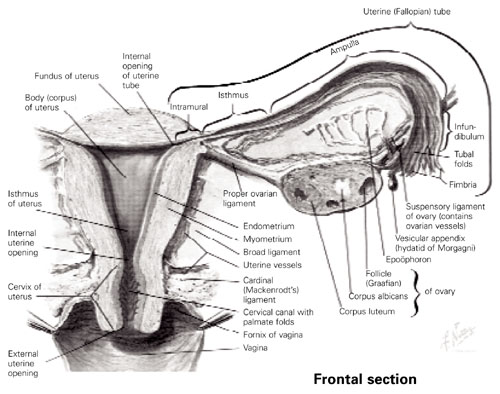
Copyright 1989. Icon Learning Systems, LLC, a subsidiary of MediMedia USA Inc. Reprinted with permission from Icon Learning Systems, LLC, illustrated by Frank H. Netter, MD. All rights reserved.
FIGURE 2 Angular versus interstitial or cornual pregnancy
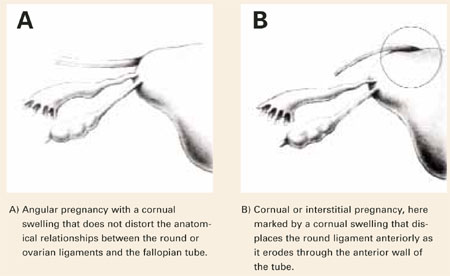
Reprinted with permission from Kadar N. Diagnosis and treatment of extrauterine pregnancies. New York: Raven Press; 1990:148.
FIGURE 3 Interstitial heterotopic pregnancy

Intraoperative photograph of an interstitial heterotopic pregnancy, with rupture of its interstitial gestation through the left salpingectomy site (located between sutures). The interstitial pregnancy is easily distinguished from an angular pregnancy by its lateral location to the ipsilateral round ligament (held in background by far babcock clamp).
Reprinted with permission from Dumesic DA, Damario MA, Session DR. Interstitial heterotopic pregnancy in a woman conceiving by in vitro fertilization after bilateral salpingectomy. Mayo Clin Proc. 2001;76:90-92.
Treatment
Any treatment of an eccyesis in a heterotopic pregnancy must consider the viability of the intrauterine pregnancy. The choice of surgical or medical treatment depends upon the hemodynamic status of the patient and the expertise of the physician. Surgical therapy is optimal when the patient is in shock and the physician has appropriate surgical training.
Surgical. While prospective randomized trials of surgical versus medical strategies do not exist, laparoscopy is ideally suited to remove an unruptured eccyesis without disrupting the remaining intrauterine pregnancy. When the eccyesis ruptures, the intrauterine gestation still can survive. But decreased perfusion to the normal pregnancy places it at theoretical risk for miscarriage.
Laparoscopy should be performed without the use of an intracervical uterine manipulator, with the Veress needle inserted carefully into the abdomen to avoid perforating the gravid uterus. After abdominal insufflation, the choice of laparoscopic salpingectomy or cornual resection depends on the location of the eccyesis within the fallopian tube or its remnant. Generally, physicians should perform a salpingectomy for ampullary pregnancies and a cornual resection for cornual pregnancies. Regardless of the surgical approach, the use of sutures3 or staples12—rather than electrocautery or intramyometrial injection of vasopressin—minimizes the risk of diminishing blood flow to the surviving intrauterine pregnancy, particularly during cornual resection. Exploratory laparotomy is appropriate when a ruptured eccyesis is associated with severe intra-abdominal hemorrhage.
Medical. Therapeutic treatments for heterotopic pregnancy include transvaginal injection of the unruptured eccyesis with potassium chloride,13 potassium chloride with methotrexate,14 or hyperosmolar glucose.15 While clinical experience in treating heterotopic pregnancy is limited, transvaginal injection of methotrexate into an eccyesis could potentially harm the adjacent intrauterine pregnancy.16 Under similar circumstances, the use of potassium chloride has been shown at the time of cesarean section to distort the cornua, suggesting longterm impairment of tubal function.11
In general, we favor the surgical therapies described above, because they can be performed quickly under outpatient conditions while eliminating the risk of later ectopic rupture. Medical therapy is best performed when the patient is clinically stable, compliant, and willing to be monitored over time in the clinic. When such a patient has restricted surgical access to the pelvis due to adhesions, we prefer administering a transvaginal injection of potassium chloride.
Final thoughts
It is important to note that one-third of intrauterine pregnancies accompanying heterotopic pregnancy miscarry in the first (89%) and second trimesters (8.5%). Miscarriage beyond the second trimester is rare, though preterm delivery may occur—particularly when heterotopic pregnancy is accompanied by multiple births. Still, a full two-thirds of intrauterine pregnancies accompanying heterotopic pregnancy do survive to term.
Early diagnosis is the key to successful treatment and delivery. Ultrasonographers must methodically examine the entire pelvic region, particularly in women who have had pelvic surgery, PID, or who are conceiving after a workup for fertility. Once a woman has been treated for interstitial or cornual heterotopic pregnancy, close observation of the patient’s hemodynamic status during labor is recommended, since the risk of uterine rupture is unknown.3
